Introduction
Lumbar hernias are among the rarest forms of abdominal wall hernia, accounting for less than 1.5% of all abdominal hernias, with fewer than 300 cases described in the literature worldwide [1]. They occur through defects in the posterior abdominal wall, most commonly in the superior lumbar triangle (Grynfeltt–Lesshaft), and less frequently in the inferior lumbar triangle (Petit’s) [2]. The superior triangle is bounded superiorly by the 12th rib, anteriorly by the internal oblique, and posteriorly by the quadratus lumborum and erector spinae muscles, and is covered by the latissimus dorsi [3].
Lumbar hernias may be congenital or acquired, with the latter further categorized as primary (spontaneous) or secondary to trauma, infection, or prior surgery [4]. Reported cases usually involve men, are left-sided, and most often contain retroperitoneal fat as the herniating tissue [5].
Because of their rarity and subtle clinical presentation, lumbar hernias are frequently overlooked or misdiagnosed, leading to delays in appropriate management. In this report, we describe an uncommon presentation of a right-sided superior lumbar hernia in an elderly Indian woman, containing omentum and occurring after trauma. This case is notable because it deviates from the typical demographic and anatomical patterns described in the literature, thereby broadening current understanding of this rare entity and underscoring the importance of maintaining a high index of suspicion in atypical patient groups.
Case report
Case presentation: A 74-year-old woman presented to the outpatient department with a swelling over the right lower back (Figure 1) of five months’ duration, associated with dull aching pain for two months. She gave a history of blunt trauma to the same region following a road traffic accident one year earlier.
The swelling was non-progressive, reduced when lying prone, and was not associated with fever, weight loss, discharge, or bowel/urinary disturbances. She was a homemaker from an upper-lower socioeconomic background, with no comorbidities or relevant family history. Her only past surgery was an open tubectomy four decades ago, after five uneventful vaginal deliveries.
Management and outcome
Given her symptoms and imaging findings, elective surgical repair was undertaken. Under general anesthesia, a right-sided oblique lumbar incision was made. The thoracolumbar fascia was incised (Figure 3), and the hernial sac was dissected from surrounding tissue. The herniated omental fat was reduced and the fascial defect closed. Reinforcement was achieved using a 5×5 cm polypropylene mesh placed in an extraperitoneal plane. Interestingly, a small adjacent lipoma (2×1 cm) was also excised.
The patient’s postoperative recovery was uneventful, and she was discharged on the fourth day. At 3-month follow-up, she remained asymptomatic with no evidence of recurrence or complications.
On examination, she was stable and systemically well. An ovoid swelling measuring 3×2 cm was noted on the right flank, 6 cm above the iliac crest and 7 cm lateral to the midline, just below the 12th rib. The swelling was soft, non-tender, reducible, and exhibited a cough impulse. Overlying skin was normal. Differential diagnoses considered included lumbar hernia, lipoma, soft tissue tumor, hematoma, abscess, and traumatic pseudohernia of the lumbar region [6].
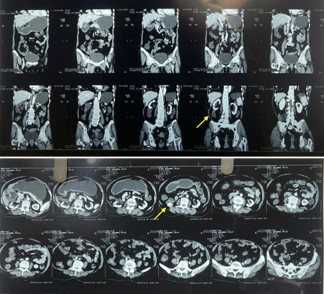
Investigations: Ultrasonography of the abdomen showed a 1.6 cm fascial defect in the posterior abdominal wall with herniation of omental fat, and a 1.3×2.9 cm hypoechoic lesion in the right lumbar region. Contrast-enhanced CT confirmed a 1.4 cm defect in the right superior lumbar triangle with a hernial sac measuring 6.5×2.4×8.3 cm extending from T11 to L2, containing omental fat (Figure 2). Notably, no bowel loops were involved. Additional findings included gallbladder sludge and benign renal cysts. Routine hematological and biochemical investigations were within normal limits. Preoperative cardiac evaluation revealed mild cardiomegaly with a small pericardial effusion but preserved function.
Discussion
Lumbar hernias are an uncommon entity, comprising less than 1.5% of all abdominal wall hernias, with most cases reported on the left side and in men [3]. The superior lumbar triangle (Grynfeltt–Lesshaft’s space) is more frequently involved than the inferior triangle [1]. Reported hernia contents include retroperitoneal fat, colon, kidney, and spleen; however, omental herniation is relatively uncommon [7].
Our case is noteworthy for several atypical features. First, it occurred on the right side in an elderly female, contrasting with the male and left-sided predominance described in literature. Second, the hernia followed a history of blunt trauma, suggesting an acquired, secondary etiology. While trauma-induced lumbar hernias have been described, delayed presentation in this demographic is rare. Third, the herniated content in our patient was omentum rather than retroperitoneal fat, which is less commonly reported. An additional lipoma in proximity to the defect further complicated the presentation.
Diagnosis can be challenging because lumbar hernias present as subtle flank swellings and may be mistaken for lipomas, abscesses, or hematomas. In this case, the differentials included pseudohernia of the lumbar region, highlighting the risk of misdiagnosis. Cross-sectional imaging, particularly CT, remains the gold standard for diagnosis, as it precisely delineates the fascial defect and contents [8].
Surgical repair is the treatment of choice in symptomatic patients to prevent complications such as incarceration or strangulation. Both open and laparoscopic approaches are described, with mesh reinforcement recommended to reduce recurrence. In our patient, an open mesh repair was performed, with good postoperative outcome and no recurrence at 3 months.
This case emphasizes the importance of considering lumbar hernia in the differential diagnosis of atypical flank swellings, particularly in elderly women with prior trauma, where clinical suspicion may otherwise be low. Awareness of such atypical presentations can prevent delays in diagnosis and management.
While this case report does not document a novel presentation, it emphasizes the clinical relevance of including lumbar hernia in the differential diagnosis of lumbar pain among elderly patients which could lead to prompt response and prevent catastrophic complications.
Conclusion
Lumbar hernias, though rare, must be considered in the differential diagnosis of flank swellings, especially in elderly patients with a history of trauma. Timely imaging and early surgical repair with mesh placement ensure excellent prognosis and minimal risk of recurrence.
Declarations
Consent to participate: Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Consent for publication: Consent of the patient and authors was obtained for publication.
Competing interests: We declare no competing interests.
Author’s contributions: All authors contributed to the report’s conception and design. The first draft of the manuscript was written by Arjun Santosh Menon and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
References
- Sharma P. Lumbar hernia. Med J Armed Forces India. 2009; 65: 178–9.
- Suh Y, Gandhi J, Zaidi S, Smith NL, Tan MY, Khan SA. Lumbar hernia: a commonly misevaluated condition of the bilateral costoiliac spaces. Transl Res Anat. 2017; 8–9: 1–5.
- Munoz-Munoz M, Torres-Mansur R, Torres-Ramirez MA. The rarity of Petit’s hernia: a case report on diagnosis and treatment. Int J Surg Case Rep. 2023; 111: 108886.
- Roham A, Gardner P, Heller J, Gerken J, Lumley C. Reconstruction of traumatic lumbar hernias: a case report. Int J Surg Case Rep. 2018; 49: 153–7.
- Walgamage TB, Ramesh BS, Alsawafi Y. Case report and review of lumbar hernia. Int J Surg Case Rep. 2015; 6: 230–2.
- Kumar S, Kumar A, Raghupathi L. Primary lumbar hernia: a rarely encountered ventral hernia. Int Surg J. 2020; 7: 1669–9.
- Lavudya G, Sainatham C, Komarapu L, Ramavath K, Mohankumar HRH, Sreepadagh N. The primary lumbar hernia with multiple defects: a rare case. Int Surg J. 2021; 9: 226.
- Guennouni A, Laridi A, Abourak C, Bahha S, Moatassim Billah N, Nassar I, et al. Lumbar hernia Jean-Louis Petit: a case report and literature review. Radiol Case Rep. 2025; 20: 4579–82.