Introduction
Rectal strictures secondary to Inflammatory Bowel Disease (IBD) are rare and typically respond to medical and endoscopic management. Surgical resection is reserved for cases with refractory symptoms, failed conservative treatment, or suspected malignancy. This report presents a complex case of chronic proctitis evolving into a low-lying rectal stricture with obstructive symptoms and nutritional compromise that ultimately required definitive surgical management via Abdominoperineal Resection.
Case presentation
Patient profile
• Age/Sex: 58-year-old male
• Medical history: Hypertension and prior hemorrhoidal disease.
Clinical presentation
The patient reported a 3-to 4-month history of alternating loose stools, constipation, indigestion, and frequent rectal bleeding. The initial laboratory test results were within the normal limits.
Initial diagnostic workup (February 2025)
• Contrast-enhanced computed tomography imaging Diffuse thickening of the large bowel, rectum, mesorectum, and anal canal suggestive of inflammation.
• Endoscopy: Colonoscopy with biopsy confirmed an inflammatory aetiology consistent with IBD.
Subsequent clinical course (May 2025)
Despite medical management and repeated hospitalizations, the symptoms persisted. A second CECT and colonoscopy revealed features of early bowel obstruction. The patient was switched to a liquid diet under dietician guidance to mitigate complications.
Stricture evolution
Digital rectal examination became increasingly limited, with palpable assessment restricted to 4 cm from the anal verge, indicating progressive stricture. Repeat imaging and biopsies continued to support an inflammatory origin, without malignancy.
Surgical management
Given the refractory nature of symptoms and the development of a low-lying stricture, multidisciplinary consensus has favoured surgical intervention. Serial dilatation was considered but deemed unsuitable because of the patient’s nutritional anaemia and obstructive signs.
Intraoperative findings
Dense adhesions were noted between the rectum and adjacent structures, including the prostate and the anterior rectal wall. The iliococcygeal ligament was divided to facilitate mobilization. However, a sphincter-preserving procedure is not feasible, necessitating the use of APR.
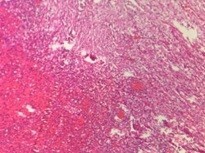
Resected specimen
Included the sigmoid colon, rectum, anal canal, perineal tissue, and the skin. Histopathology confirmed chronic proctitis with dense lymphoplasmacytic infiltrates, crypt distortion, and focal neutrophilic activity. No dysplasia or malignancy was observed in any patient.
Postoperative course
Recovery was uneventful. Minor postoperative complications were managed conservatively. The patient resumed oral intake and was discharged on day 15. Follow-up every three months was recommended.
Discussion
This case underscores the potential for chronic inflammatory colitis to progress to a clinically significant rectal stricture with obstructive symptoms. Despite appropriate medical treatment, the disease has evolved, necessitating surgical intervention. APR, typically reserved for malignancy, is essential in this refractory inflammatory scenario. Dense adhesions and altered anatomy preclude sphincter preservation. Early recognition and timely surgical management are critical in such cases, especially when the nutritional status deteriorates.
Conclusion
In patients with refractory proctitis and progressive rectal strictures, APR may be warranted when conservative measures fail. Comprehensive preoperative evaluation and multidisciplinary planning are vital. Regular postoperative monitoring ensures optimal recovery and early detection of complications.
Declarations
Conflict of interest statement: The authors declare no conflicts of interest related to this case report.
Data access statement: All the data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethical statement: Informed consent was obtained from the patient for publication of this case report and accompanying images. The institutional ethical guidelines were followed.
Funding statement: No external funding was received for the preparation of this manuscript.
References
- Fehily SR, Martin FC, Kamm MA. Simple novel tacrolimus enemas are very effective in severe refractory proctitis. J Crohns Colitis. 2019; 13: S402.
- Raja SS, Bryant RV, Costello SP, et al. Systematic review of therapies for refractory ulcerative proctitis. Practical Gastroenterology. 2021.
- Garcia-Henriquez N, Galante DJ, Monson JRT. Selection and outcomes in abdominoperineal resection. Front Oncol. 2020; 10: 1339.
- Choi MS, Yun SH, Shin JK, et al. Single-port robot-assisted abdominoperineal resection: a case review of the first four experiences. Ann Coloproctol. 2022; 38: 88–92.
- Albano MN, Louro JM, Brito I, Ramos S. Perineal reconstruction using an inferior gluteal artery perforator flap after abdominoperineal resection. BMJ Case Rep. 2019; 12: e228613.
- Heald RJ, Ryall RD. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet. 1986; 1: 1479–82.
- Miles WE. A method of performing abdomino-perineal excision for carcinoma of the rectum and of the terminal portion of the pelvic colon. Lancet. 1908; 2: 1812–3.
- Wexner SD, Duthie GS. Surgical treatment of ulcerative colitis and refractory proctitis. In: Wexner SD, Duthie GS, editors. Colorectal Surgery. London: Springer. 1999.
- Gorfine SR, et al. Persistent perineal sinus after APR: management strategies. Dis Colon Rectum. 2005; 48: 2052–7.