Introduction
A 28-year-old male presented to the emergency department with intractable vomiting and retrosternal chest pain on a background of poorly controlled type 1 diabetes mellitus. Laboratory investigations demonstrated a neutrophilic leukocytosis as well elevated blood glucose (18) and ketones (4.6), serum lactate was normal at 1.2. A diagnosis of evolving diabetic ketoacidosis was made and initial management with glucose control and hydration commenced.
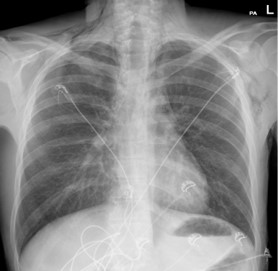
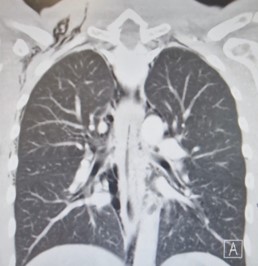
A chest X-ray performed (Figure 1) in the Emergency Department demonstrated significant subcutaneous emphysema. Subsequent computed tomography of the thorax showed extensive pneumomediastinum with a locule of intramural gas possibly reflecting a focal rupture point (Figure 2).
An emergency Oesophagogastricduodenoscopy (OGD) was performed which demonstrated a black oesophagus with an abrupt and striking cut-off at the oesophagogastric junction (Figure 3). A diagnosis of Ecute Esophageal Necrosis (AEN) was made.
The patient was managed conservatively with bowel rest and total parenteral nutrition for a total of 2 weeks. A gastrograffin swallow was performed after 7 days demonstrated no persistent leak. A repeat OGD 14 days later demonstrated a marked improvement with near complete resolution (Figure 4).
Although a rare entity, AEN should be considered in the setting of chest pain especially on a background of diabetes mellitus and intractible vomiting. Failure to diagnose and commence appropriate management can result in significant morbidity and mortality. Oesophageal stricture formation is seen in up to 10% of patients following AEN, therefore adequate clinical follow-up is vital.