Introduction
Desmoid-type fibromatosis, is a rare soft tissue tumor with the typical clinical behavior of frequent local recurrence without distant spread [2]. The main locations include the mesentery, the abdominal wall, and the extremities [3]. The incidence is approximately 0.2% of all neoplasms of the breast [2,4]. The main risk factors are trauma and surgery, as well as being an association with Gardener’s syndrome [5,6]. Some have suggested that this entity arises from within the breast parenchyma itself, while others have suggested that it arises from the aponeurosis overlying the pectoralis major muscle [4,9]. According to the current consensus from existing research, e.g., of the Desmoid Tumor Working Group and ESMO, active primary surgical therapy is no longer the method of choice for asymptomatic patients [4,7,8], however surgical excision with wide margins remains a valuable therapeutic option, especially in symptomatic and progressive desmoid type fibromatosis or impaired quality of life to avoid recurrence of this locally aggressive tumor [3].
The current report aims to report a rare case of desmoid type fibromatosis of the breast. The report has been arranged in line with SCARE guidelines with a brief literature review [1].
Patient case presentation
Patient information
A 33-year-old Saudi female, married, not known to have chronic medical illness, was referred in January 2024 to breast oncoplastic clinic in king Saud medical city NGHA in Jeddah, KSA, for a painless left breast lump that is increasing in size over 2 months, without skin or nipple changes or discharge.
Patient denied any history of trauma, family history of breast cancer, previous breast surgery.
Clinical findings
Bilateral asymmetrical breasts, the right breast was bigger, Size D cup, grade 2 ptosis, Left breast: unifocal around 1 x 1 cm palpable non tender mass at 3 o’clock, firm, not attached to the skin or chest wall.
Diagnostic assessment and interpretation
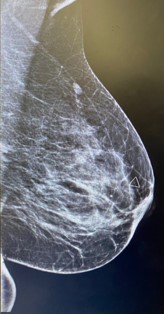
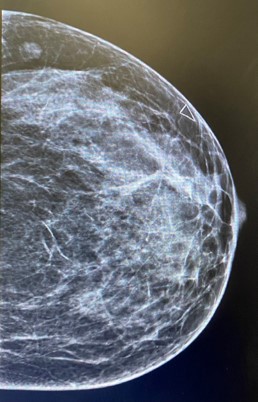
Left breast and axilla ultrasound and Mammogram showed: Left breast palpable lesion with architectural distortion in the upper lateral mid/anterior third at 3:00, It measures 0.9 cm and seen with no significant vascularity. A clip was placed.
Left breast, vacuum assisted biopsy of the indexed lesion showed: Infiltrating bland looking spindle cells proliferation in long sweeping fascicles that are partially positive for betacatenin immunostaining, suggestive of desmoid fibromatosis.
Immunohistochemistry study: The spindle cells are partially positive for Beta-catenin (nuclear staining), focal positive for SMA, while negative for PAN CK, CK5/6, P63, CD34.
Intervention
Once a diagnosis was established, surgery was scheduled. The patient was taken to the operating room for Left breast conserving surgery.
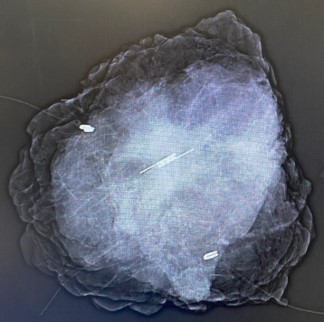
Which performed under general anesthesia with selective intubation intraoperative mammogram was done after the resection confirming the clip at the center of the specimen.
The left wide local excision site was then closed in a standard manner. No attempts at cosmetic breast reconstruction with autologous tissue transfer or expander/implant placement were considered at that time.
The surgically removed specimen was weighing 44.4 grams and measuring 5.5 × 4.9 × 2.8 cm, with grossly tan-white, firm mass with irregular border, The specimen was sent to histopathology department in formalin.
Follow up and outcome
Histological evaluation of the surgical specimens revealed desmoid type fibromatosis with tumor size 1.5 cm in greatest dimension, tumor extent, infiltration into the surrounding adipose tissue with entrapped benign mammary ducts, margin status.
All negative for tumor and distance from closest margin: 4 mm from inferior margin.
The post-operative course was uneventful, and the patient was discharged home at the same day, seen in the clinic week after, wound asset it was well healed.
Case was discussed in the tumor board; decision was toward no further treatment is required
CT CAP done as a part of the work up, findings on the intrathoracic and intra-abdominal organs were physiological.
Discussion
World Health Organization (WHO) defined desmoid type fibromatosis as an intermediate soft tissue tumor with the characteristic of clonal fibroblastic proliferation derived in the deep soft tissue with the ability of local infiltration [2]. Fibromatosis is a rare tumor with locally aggressive behavior and high incidence of local recurrence. The reported risk factors include surgical trauma, silicone implants in addition to its association with Gardener’s syndrome [6]. Clinically, this tumor manifests as a broad spectrum and in most cases, desmoid type fibromatosis of the breast is described as a suspicious, mobile, firm, and painless nodule [5].
Mammography presents irregular walled and highly dense lesion with no calcifications mimicking sometimes breast carcinoma [6].
Radiologic evaluation of our case revealed soft tissue mass inducing architectural distortion.
Histopathological examination is crucial for diagnosis, and often revealing spindle cells with minimal cytological atypia and abundant collagenous matrix [4]. A diagnosis can be made from microscopic findings on routine hematoxylin and eosin-stained sections. Furthermore, immunohistochemical staining for β-catenin with nuclear positivity is also useful in establishing a diagnosis, but there are no specific immunomarkers for breast fibromatosis [2].
In conclusion, fibromatosis represents a diagnostic and therapeutic challenge due to its infiltrative nature and propensity for recurrence. A multidisciplinary approach involving oncologists, surgeons, and radiologists is crucial for optimal management. Further research is needed to elucidate the molecular pathways driving fibromatosis and to develop targeted therapies that can improve outcomes while minimizing morbidity.
Conclusion
Due to the rare involvement of the breast in patients with desmoid-like fibromatosis, the present study reports this case with its clinical feature and histological finding to improve and add to our knowledge of the disease.
Declarations
Human subjects: Patient informed consent was obtained.
Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work.
Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work.
References
- Bhangu A, Fitzgerald JE, Soreide K, Rey-Bellet O, Feroci F, Tolonen M, et al. The SCARE 2023 guideline: updating consensus Surgical CAse REport (SCARE) guidelines. Int J Surg. 2023; 109: 106990.
- Haubner F, Ohmann E, Pohl F, Strutz J, Gassner HG. Wound healing after radiation therapy: Review of the literature. Radiat Oncol. 2012; 7: 162.
- Wang Y, Chen X, Liu Y, Tan X, Li X, Zhang H, et al. The Role of Ultrasound in Diagnosis and Evaluation of Desmoid-Type Fibromatosis. Front Oncol. 2021; 11: 630555.
- Chu CH, Chen PC, Hsieh TJ, Lin YC, Kao YL, Tsai KL, et al. Breast fibromatosis: Imaging findings and literature review. J Med Ultrasound. 2021; 29: 243–8.
- Tian H, Pan J, Chen L, Wu Y. A narrative review of current therapies in unilateral recurrent laryngeal nerve injury caused by thyroid surgery. Gland Surg. 2022; 11: 270–8.
- Abbas AE, Deschamps C, Cassivi SD, Nichols FC, Allen MS, Pairolero PC. Chest wall desmoid tumors. Ann Thorac Surg. 2004; 77: 169–72.
- Nuyttens JJ, Rust PF, Thomas CR Jr, Turrisi AT 3rd. Surgery versus radiation therapy for patients with aggressive fibromatosis or desmoid tumors: A comparative review of 22 articles. Cancer. 2000; 88: 1517–23.
- Kasper B, Baumgarten C, Garcia J, Bonvalot S, Haas R, Haller F, et al. An update on the management of sporadic desmoid-type fibromatosis: A European Consensus Initiative between Sarcoma Patients EuroNet (SPAEN) and European Organization for Research and Treatment of Cancer (EORTC)/Soft Tissue and Bone Sarcoma Group (STBSG). Eur J Cancer. 2020; 127: 159–72.
- Shields CJ, Winter DC, Kirwan WO, Redmond HP. Desmoid tumours. Eur J Surg Oncol. 2001; 27: 701–6.