Ten rules of doing laparoscopic completion cholecystectomy
Nachiket Rahate*
Kasturba Hospital, Manipal Academy of Higher Education, India.
Kasturba Hospital, Manipal Academy of Higher Education, India.
Sub-total cholecystectomy is bail out procedure for difficult Gall bladder surgery. Long term sequalae can be remnant Gall bladder cholecystitis and stone disease which needs completion cholecystectomy. Certain rules are to be followed during this surgery: adhesiolysis, skeletonization, judicious use of energy, NIR imaging, posterior window formation, empty the GB when needed, avoid spillage of bile, proper haemostasis, anatomy delineation, keep biliary ducts in vision. This will prevent billio-vascular catastrophe.
Manuscript Information: Received: Apr 12, 2025 Accepted: May 27, 2025 Published Online: Jun 03, 2025
Journal: Annals of Surgical Case Reports & Images
Online edition: https://annscri.org
Copyright: © Rahate N (2025). This Article is distributed under the terms of Creative Commons Attribution 4.0 International License.
Cite this article: Rahate N. Ten rules of doing laparoscopic completion cholecystectomy. Ann Surg Case Rep Images. 2025; 2(1): 1083.
Due to previous inflammatory response and surgery, there are always lot of adhesions near the gall bladder remnant. Duodenum, colon and omentum are frequently adhered to the area. Gentle and meticulous dissection either by sharp dissection by scissors or judicious use of energy source like ultrasonic dissector done. Care should always need to prevent enterotomy and vasculobiliary injury.


One needs expertise in treating hilar vasculobiliary injuries while attempting for such surgeries. NIR imaging helps a lot. ICG dye can be given 90 min before surgery. A radio marked gauze piece is always handy to give traction and stop small oozers by compression.
One needs expertise in treating hilar vasculobiliary injuries while attempting for such surgeries. NIR imaging helps a lot. ICG dye can be given 90 min before surgery A radio marked gauze piece is always handy to give traction and stop small oozers by compression.
With meticulous and slow dissection, once remanent gall bladder is identified, all fibro-fatty tissues over gall bladder and callots area is skeletonized taking help of NIR imaging. skeletonization helps in better NIR imaging.
Is the key to prevent complications in this surgery. use of only scissors or small bursts of energy like ultra-sonic dissector or bipolar energy is rule. Giving traction and countertractions by atraumatic grasper can find proper plains of dissection.

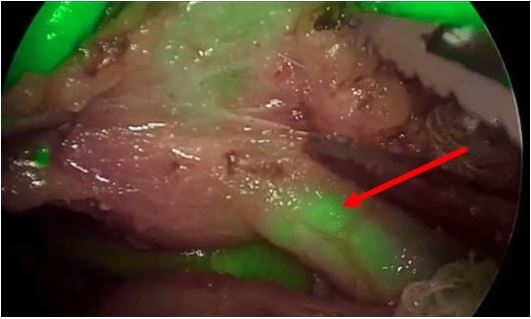
ICG dye should be injected 90 min prior to surgery. NIR imaging helps in identifying the biliary structures and non-biliary structures. This prevents biliary injuries during dissection. In case of doubt, 2 ml intravenous ICG dye can be given as bolus to identify vascular anatomy. Care should always be taken to prevent bile leak in the area. bile leak nulls the NIR imaging.
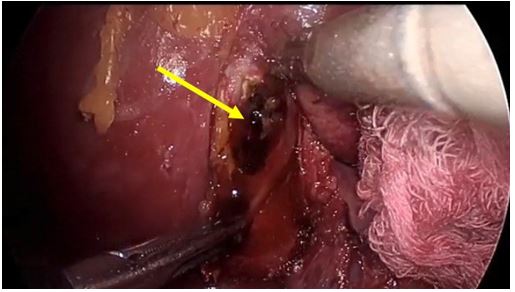
As is the rule of laparoscopic cholecystectomy, posterior window creation should always be tried. Sometimes due to dense adhesions and small size of remnant gall bladder, posterior dissection becomes technically difficult. Creation of critical view of safety helps in safe cholecystectomy in such cases.

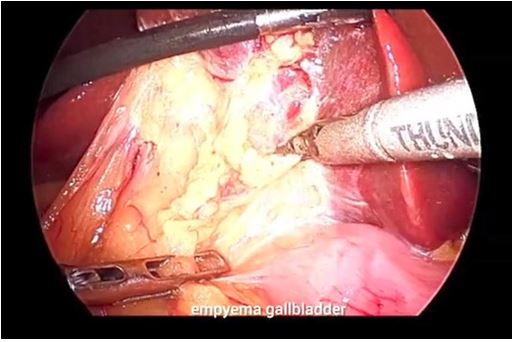
Sometimes the small remnant gall bladder is thickened and studded with stones. In such situations better to open the gall bladder near the fundus and empty all containts. This makes gall bladder supple and easy to handle. This step shortens the surgical time. But this can lead to bile staining of tissues and prevents identification of biliary structures. Gauze piece kept in the vicinity can soak the bile containts.

Blood will stain the tissues and make job difficult. Dissection plains will be difficult to find. Bile staining will make staining of tissues by ICG Dye and this will make biliary anatomy obscure to identify. Hence proper haemostasis and preventing bile leak will keep biliary ducts in vision and one can complete the remnant cholecystectomy. If the callots dissection is too difficult to identify callots biliary structure due to fibrosis, ICG dye will also not identify the biliary structures. In such scenarios, intraoperative conventional cholangiography will help in finding the path if CD, CHD & CBD. A small 6 French size catheter is introduced through open fundus. Take purse string suture around the tube and flush the GB with radiological iodine dye. This identification of anatomy can increase the boldness of surgeon to complete the cholecystectomy. Last option is low threshold to convert the laparoscopic surgery to open. During open surgery Thompson retractor should be used to have a better vision during surgery in depth.
Proper surgical precautions at every step are extremely important while performing laparoscopic completion cholecystectomy. This surgery needs good laparoscopic vision, NIR imaging and good energy devices for dissection. Last goal of surgery is to complete safe cholecystectomy.