Introduction
Colonoscopy is used as a diagnostic and screening method for multiple digestive tract diseases with high acceptance and safety [1]. The complication rate is 0.5% [2], with intestinal perforation and bleeding being most common [1].
Spontaneous splenic rupture associated with colonoscopy is rare (1:100,000) [3] and rarely reported in medical practice. The actual incidence of this event remains unknown, with some case series reporting a variation between 0.0001% and 0.0004% [1,4,5].
Splenic Rupture (SR) after colonoscopy is clinically diagnosed, particularly in cases of severe early hemodynamic instability [1]. The main reported symptoms are intense abdominal pain, sometimes with referred pain in the left shoulder, peritonism, and hypovolemic shock [1]. Symptoms usually appear within the first 24 hours after the procedure; however, cases have been described in which symptoms manifest up to five days after colonoscopy [6].
Computed Tomography (CT) is considered the gold standard for the detection of this event [1]. In cases in which CT is not feasible, abdominal ultrasound can be used for diagnosis [7].
The treatment approach varies depending on the clinical condition of the patient and urgency of the case. Surgery is the most common choice of treatment [6] and typically involves total splenectomy. Conservative management is an alternative when the clinical picture allows, although its use has rarely been reported.
Although colonoscopy, even interventional, is considered a safe procedure, early recognition of uncommon adverse events is essential to reduce the associated morbidity and mortality. This report contributes to the literature by expanding the knowledge on the possible complications of colonoscopy and aiding clinical decision-making in similar cases.
Case report
A 64-year-old female patient underwent interventional colonoscopy for mucosectomy in the ascending and descending colons. Her medical history included dyslipidemia and hypertension with no prior abdominal surgeries. She was on chronic prednisone (5 mg/day) and tofacitinib citrate (10 mg/day) for rheumatoid arthritis. At the time of the examination, she reported no abdominal discomfort or altered vital signs.
Colonoscopy was performed without complications, and the planned mucosectomies were performed as follows: one in the ascending colon, two in the descending colon, and one in the sigmoid colon. Upon awakening from anesthesia, the patient reported no complications.
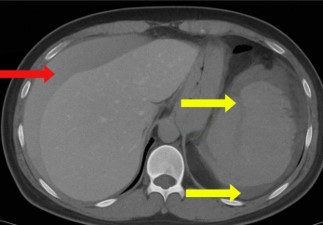
One day after the procedure, she visited the emergency department following three episodes of hematochezia and multiple episodes of near-syncope without loss of consciousness. She presented with intense abdominal discomfort, hypotension (BP=84/59 mmHg), and tachycardia (HR=110 bpm). A CT scan of the abdomen revealed a grade four splenic lesion in the middle third and free fluid in the splenic and perihepatic spaces (Figures 1 and 2).
Upon admission, laboratory tests showed a hemoglobin of 9.2 g/dL and lymphocytosis with a lymphocyte count of 17,100/ mm³. No other significant abnormalities were found.
The reported perisplenic hematoma volume was approximately 730 mL. The measured volume in the pelvic cavity was approximately 640 mL and the estimated free fluid in the perihepatic space was 250 mL. The patient was stabilized with two liters of Ringer’s lactate solution and then transferred to the operating room for total splenectomy.
During the perioperative period, one unit of packed red blood cells was infused due to the hemoglobin level (6.5 g/dL). The surgery was completed without major complications and lasted a total of 130 minutes. The resected spleen showed extensive hilar injury with capsular rupture and an adjacent hematoma (Figure 3).
Postoperatively, another unit of packed red blood cells was administered due to a hemoglobin drop to 8.1 g/dL. No further complications were noted. Laboratory tests at discharge showed no significant alterations, with a hemoglobin level of 11.5 g/dL. The total hospital stay was six days, three of which were in the intensive care unit.
Discussion
Splenic rupture during colonoscopy is an extremely rare complication, with only a few cases reported in the medical literature. This specific case highlights the importance of being aware of this possible, albeit unlikely, complication and the necessity for immediate surgical intervention.
The exact mechanism of injury is not fully understood; however, it is believed that mechanical distension of the colon, excessive endoscope movements, and splenocolonic adhesions may contribute to splenic trauma. Direct trauma to the spleen due to colonoscope manipulation is also a plausible hypothesis [8,9].
Diagnosing post-colonoscopy SR can be challenging due to its nonspecific clinical presentation, which may include diffuse abdominal pain, referred left shoulder pain (Kehr’s sign), hypotension, and signs of hypovolemic shock [9]. Abdominal ultrasound and CT are crucial tools for confirming hemoperitoneum and determining the extent of splenic injury.
Immediate treatment involves hemodynamic stabilization and emergency splenectomy in most cases. Splenic embolization can be a viable alternative in selected cases, in which the patient’s condition allows [10]. However, splenectomy remains the standard treatment due to the severity of bleeding associated with SR [8,10].
A literature review revealed that most SR cases occur in patients with predisposing conditions, such as splenic adhesions, hematologic diseases, or splenomegaly [9]. This particular case highlights the absence of obvious risk factors, emphasizing that this adverse event can occur even in patients without a significant medical history. Endoscopists must be aware of this complication, especially in patients who present with abdominal pain and hemodynamic instability after the procedure.
The interventional nature of colonoscopy (biopsies, polypectomies, mucosectomies) has not been associated with an increased risk of splenic injury [1]. A systematic review reported that 62.75% of SR cases occurred during noninterventional colonoscopies, whereas only one-third occurred during interventional procedures [2].
To minimize the risk of splenic rupture, careful handling of the colonoscope is recommended to avoid excessively aggressive maneuvers, especially near the splenic flexure. Awareness of possible splenic adhesions in patients with a history of abdominal surgery or inflammatory bowel disease is also crucial [8].
Although rare, splenic injury should be considered in the differential diagnosis of patients who present with hemodynamic instability or abdominal pain after the procedure.
Early hemodynamic stabilization, appropriate imaging, and rapid surgical decision-making were crucial for favorable outcomes in this case.
Conclusion
Splenic rupture remains a rare event despite underdiagnosis and underreporting. Among the tools used for identifying this condition, CT proved useful and effective, provided there was prior patient stabilization. The treatment is usually surgical, as seen in this case, although conservative management may be viable depending on lesion severity, patient profile, and case gravity.
Therefore, the hypothesis of SR should be considered when a patient presents with abdominal pain and hypotension after undergoing interventional procedures, such as colonoscopy. Accurate identification and appropriate management of SR are key predictors of favorable outcomes.
References
- Piccolo G, Di Vita M, Cavallaro A, Zanghì A, Lo Menzo E, Cardì F, et al. Presentation and Management of Splenic Injury After Colonoscopy. Surg Laparosc Endosc Percutan Tech. 2014; 24: 95–102.
- Cathala Esberard B, Mohseni M. Splenic injury: a rare complication of lower endoscopy. BMJ Case Rep. 2020; 13: e234440.
- Zappa MA, Aiolfi A, Antonini I, Musolino CD, Porta A. Splenic rupture following colonoscopy: Case report and literature review. Int J Surg Case Rep. 2016; 21: 118–20.
- Garcia MJ, Castañera González R, Gomez Ruiz M, Martín Rivas B, Rivero Tirado M. Splenic rupture after colorectal cancer screening. Revista Española de Enfermedades Digestivas. 2015.
- Rex DK. Colonoscopic splenic injury warrants more attention. Gastrointest Endosc. 2013; 77: 941–3.
- Barbeiro S, Atalaia-Martins C, Marcos P, Nobre J, Gonçalves C, Aniceto C. Splenic Rupture as a Complication of Colonoscopy. GE Port J Gastroenterol. 2017; 24: 188–92.
- Cappellani A, Di Vita M, Zanghì A, Cavallaro A, Alfano G, Piccolo G, et al. Splenic rupture after colonoscopy: Report of a case and review of literature. World Journal of Emergency Surgery. 2008 Dec 9; 3: 8.
- Ha JF, Minchin D. Splenic injury in colonoscopy: A review. International Journal of Surgery. 2009; 7: 424–7.
- Shankar S, Rowe S. Splenic injury after colonoscopy: case report and review of literature. Ochsner journal. 2011; 11: 276–81.
- Aleem MS, Ponnekanti S, Lamichhane B, Anwar M, Ghimire S, Kolade V. Splenic Injury After a Screening Colonoscopy. Cureus. 2022.