Pigmented villonodular synovitis (PVNS) combined with a popliteal cyst
Xinming Qi; Yi Sun; Nana Wang; Qiang Ren*
Binzhou Medical University Hospital, PR China.
Binzhou Medical University Hospital, PR China.
Pigmented Villonodular Synovitis (PVNS) is a rare proliferative disease. You are more likely to experience it as a child, but adults get sick with the same thing too. It involves mainly the synovial joints, tendon sheaths and bursa membranes; knee is most commonly affected site but hip shoulder and smaller” joints may also be involved. Usually magnetic resonance imaging or, MRI that can detect the unique features of this disease. PVNS is most commonly treated with surgery that completely excises the affected joint, thereby eliminating of abnormal tissue and reducing risk for recurrence. A 65-year-old patient with PVNS of the knee joint combined a popliteal cyst was treated by total synovectomy in this case. There was no recurrence in the condition at a two-year follow-up after surgical treatment, with improved symptoms. This case highlights the supreme importance of early diagnosis and complete surgical eradication in achieving a good long-term outcome for PVNS patients.
Keywords: Pigmented villonodular synovitis; Popliteal cyst; Arthroscopic operation.
Manuscript Information: Received: Apr 15, 2025 Accepted: May 16, 2025 Published Online: May 23, 2025
Journal: Annals of Surgical Case Reports & Images
Online edition: https://annscri.org
Copyright: © Qiang R (2025). This Article is distributed under the terms of Creative Commons Attribution 4.0 International License.
Cite this article: Xinming Q, Yi S, Nana W, Qiang R. Pigmented villonodular synovitis (PVNS) combined with a popliteal cyst. Ann Surg Case Rep Images. 2025; 2(1): 1079.
Pigmented villonodular synovitis is a rare benign proliferative disease of synovial membranes, causing villonodular synovial hyperplasia and hemosiderin deposition. Its intra-articular forms most commonly affect the knee [1]. The gold standard of treatment for pigmented villonodular synovitis has traditionally been surgical excision with total synovectomy of the affected joint. If left unaddressed, pigmented villonodular synovitis can lead to a range of complications from moderate to severe joint deformities, progressive degenerative changes in the joints, and the onset of osteoarthritis [2]. Since this condition is uncommon and frequently misdiagnosed, securing an early diagnosis with the aid of MRI scanning is of paramount importance.
In this article, we report a case of a 65-year-old patient with PVNS of the knee joint, combined with a popliteal cyst, who underwent total synovectomy. After being admitted to the hospital, the patient received a diagnostic imaging examination and subsequently underwent a surgical procedure. The outlook following the surgery is positive. Given the advanced age of the patient coupled with a popliteal cyst, the purpose of presenting this case is to underscore the occurrence of Pigmented Villonodular Synovitis (PVNS) among the elderly population and to impart our insights garnered from the diagnosis and management of PVNS.
A 65-year-old female patient has suffered pain in her right knee joint for two months. Her medication treatment was not effective, so she came to our hospital for medical consultation.
On magnetic resonance imaging of the right knee, degenerative changes and joint effusion were also noted as with a lesion in synovial membrane. The findings in the popliteal fossa were also suggestive of a popliteal cyst (Figure 1).
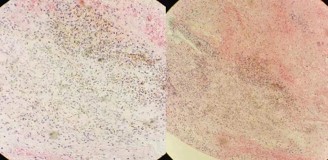
Intraoperative articular effusion was turbid, synovitis with villous proliferation Hyperemic and edematous. The surface showed obvious deposition of hemosiderin-like pigmentation (Figure 2). The pathology of synovial tissue showed that the papillary hyperplasia in surface synovial cells with an increase proliferation of fibrous tissues beneath the stretch, dilating and congesting blood vessels accompanied by tropical necrosis surrounding small veins was occasionally appeared as well as a mild chronic inflammatory cells infiltration (Figure 3). The patient was diagnosed with pigmented Villonodular Synovitis (PVNS) associated with a popliteal cyst by arthroscopy from these results.
Two years later, the patient has not shown any additional symptoms with no recurrent of previous one.

MRI of right knee joint showed degenerative changes, effusion and synovial membrane lesions in the knee joint along with presentation at popliteal fossa suggestive of a popliteal cyst.
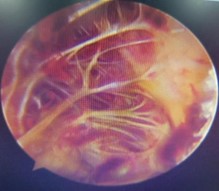
The joint fluid appearance was turbid, and the synovium exhibited villous proliferation with prominent hyperemia and edema. However, the surface showed conspicuous deposition of hemosiderin-like pigments.
Synovial cell hyperplasia on the surface, increased proliferation of fibrous tissue below, vasodilation and congestion, mild chronic inflammatory cell infiltration.
A 65-year-old patient with Pigmented Villonodular Synovitis (PVNS) of the knee joint and popliteal cyst. Although pigmented villonodular synovitis is commonly found in children, this case report demonstrates that it can also present in the elderly. Lesions are most commonly found in the knee joint, accounting for 66% to 80% of cases, with the hip, ankle, shoulder, and elbow joints following in frequency [3]. The findings on radiographs are usually non-specific, and there are no significant changes in bone density or in the joint space until the later stages of the disease. As it progresses, evidence of bone erosion may appear, manifesting as subchondral bone deficits and erosions at the margins of the joints—these are hallmarks of osteoarthritis. MRI provides significant benefits for the diagnosis and management of PVNS [3]. It is a highly effective tool for evaluating musculoskeletal structures. Moreover, it provides accurate data of the lesions preoperatively and aids in monitoring for disease recurrence [4].
The joint fluid typically appears dark brown or blood-stained due to hemosiderin deposition, and the synovium shows diffuse thickening with numerous villous and nodular processes. The diagnosis of the disease can be confirmed by histopathology.
The main treatment for PVNS is surgical resection. This treatment method can inhibit the progression of the disease and improve joint function [5]. For the patient, we have opted for the less invasive arthroscopic surgery.
For this disease, we recommend early intervention. The patient has developed a popliteal cyst, so we reasonably suspect that the cyst may be caused by PVNS, making early diagnosis and intervention particularly important.
Patient’s consent: Informed consent was obtained from the patient.
Competing interest: The authors declared no conflict of interest.
Contributors: RQ QXM and SY conceived and planned the study. RQ took the lead in writing the manuscript. QXM SY and WNN significantly contributed to drafting and revision of the paper. RQ QXM SY and WNN were main treating physicians of studied patient. All authors approved the final version.