Background
GISTs are rare mesenchymal neoplasms that arise from the interstitial cells of Cajal, specialized network-forming cells distributed in the smooth muscle wall of the digestive tract with a pacemaker role. Regarding the Gastrointestinal (GI) tract, GIST are the most common sarcoma representing 0.1-3.0% of all GI neoplasms [1]. The most common localization of GISTs is the stomach (60%), 30% are in the jejunum and ileum, 5% in the duodenum, 4% in the colorectum, and a few have been reported in the esophagus and appendix [2,3].
The latest 2020 World Health Organization (WHO) Classification of STS and bone sarcoma codes all GISTs, regardless of size, site of origin, and mitotic index, as malignant [4].
The clinical presentation of GISTs is often nonspecific and may mimic common GI diseases. Patients may experience abdominal pain, bloating, early satiety, nausea and vomiting, and iron deficiency anemia. This last symptom is not only frequent after bariatric surgery but is also a key clinical indicator of Esophagogastric (EG) cancer, which could be masked by the iron supplementation recommended after the majority of bariatric procedures. In some cases, GISTs can remain asymptomatic until they reach a substantial size or metastasize. This highlights the importance of maintaining a high index of suspicion and conducting a thorough evaluation in bariatric patients with GI complaints.
The growth stimulation of GISTs is provided by identified mutations of c-KIT, PDGFRA, and BRAF genes, found in 85%, 5%, and less than 1% of cases, respectively [5].
The incidence of GISTs is 10-15 cases per million worldwide [6]. They can occur at any age, but they are more frequently diagnosed in individuals aged 50-70 years [5].
− The diagnostic workup for detecting lesions could include: Computed Tomography (CT), which represents the gold standard for evaluating abdominal masses, as it provides information about the size, location, and presence or absence of regional and distant spread [7]. In addition, the use of intravenous contrast improves the evaluation of the tumor margins.
− Magnetic Resonance Imaging (MRI) may provide more information on internal features of the tumor, such as hypervascularity, and is also better at detecting liver metastasis [8].
− Endoscopic Ultrasound (EUS) may be helpful because most GISTs arise within the muscularis propria and appear as submucosal or mural masses [9]. EUS assessment is the standard approach for patients with oesophagogastric or duodenal nodules <2 cm [10].
− [18F]2-Fluoro-2-deoxy-D-Glucose (FDG) uptake using an FDG–Positron Emission Tomography (PET) scan, or FDG–PET-CT/MRI, may be useful, mainly when early detection of the tumor response to molecular-targeted therapy is of special interest or when surgical resection of metastatic disease is considered [11].
− Esophagogastroduodenoscopy (EGDS) with biopsy is crucial for assessing the tumor’s location within the GI tract and obtaining tissue samples for histological confirmation.
− Histopathology often reveals characteristic spindle or epithelioid cells with immunohistochemical markers like CD117 (c-kit) and CD34 [5].
According to ESMO-EURACAN-GENTURIS guidelines, the standard treatment for localized GISTs is complete surgical excision of the lesion, with no dissection of clinically negative lymph nodes. The goal is R0 excision, meaning that the excision should have margins clear of tumor cells, at least at the site of origin in the GI tract. In cases of low-risk GISTs located in unfavorable locations, the decision can be made with the patient to possibly accept R1 (microscopically positive) margins.
Imatinib, the first tyrosine kinase inhibitor, is the standard treatment for locally advanced, inoperable, and metastatic patients. This treatment is recommended except for GISTs without KIT/PDGFRA mutations or those with a PDGFRA exon 18 D842V mutation. It is also indicated for patients with a significant risk of relapse [10].
Postoperative care for GISTs is not standardized due to insufficient data. Relapses occur more frequently in the liver and/or peritoneum. Bone lesions and other sites of metastasis may be less common during the course of metastatic disease treated with several lines of therapy. The speed at which relapses take place is likely affected by the mitotic rate. Risk assessment based on the mitotic count, tumor size, and site may be useful in determining the routine follow-up policy. High-risk patients often experience a relapse within 1-3 years after the end of adjuvant therapy, while low-risk patients may experience a relapse later [10].
Monitoring for complications, such as leaks or strictures, is essential, especially when dealing with previous bariatric procedures. Furthermore, long-term follow-up is critical, as GISTs have the potential for recurrence or metastasis. This necessitates close surveillance through imaging studies and clinical evaluation.
Case presentation
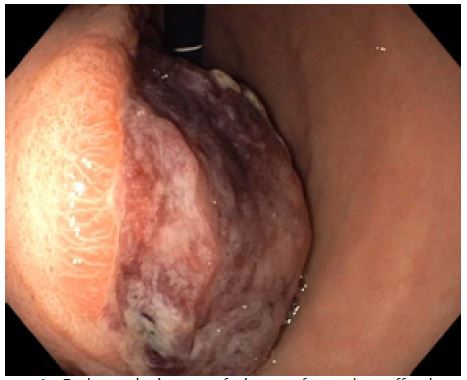
A 57-year-old woman with a history of hypertension, depressive syndrome, right hemithyroidectomy, and several bariatric procedures (Table 1) was hospitalized in the Internal Medical Unit of our clinic for an episode of acute anemia (hemoglobin 79 g/L). She had a well-known iron deficiency anemia that had been present for one year and was being treated with iron carboxymaltose. During the hospitalization, she received transfusions of packed red blood cells, and an Esophagogastroduodenoscopy (EGDS) was performed. It revealed a bulky, vegetant, ulcerated neoformation affecting the angulus/anterior wall of the stomach (Figure 1). The neoformation was sampled with biopsy forceps, and it was histologically defined as a superficially eroded hyperplastic polyp. The Helicobacter Pylori was negative on histological examination (Figure 1).
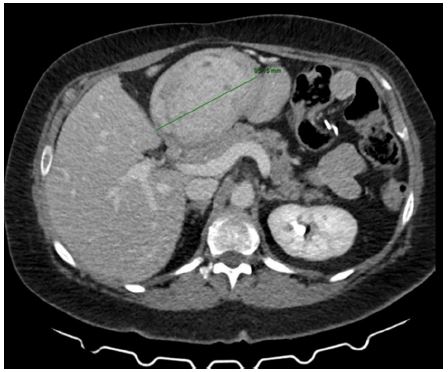
Subsequently, a staging CT scan with iodinated contrast medium confirmed the presence of the large stomach neoformation (9.5 cm in diameter) with an exophytic development (Figure 2). It was suspected to be a GIST and was in contact with the left hepatic lobe, the intra-abdominal wall, the pancreas, and the duodenum, without any lymphadenopathies or signs of possible metastasis (Figure 2).
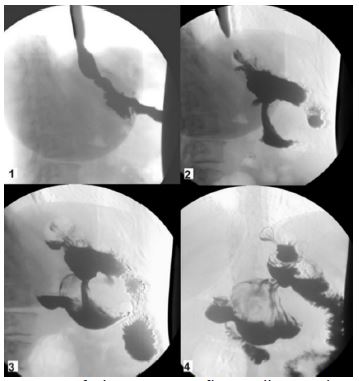
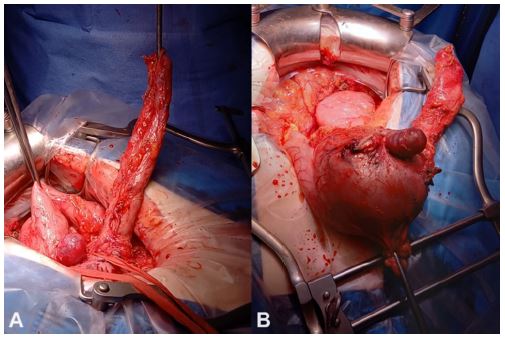
After multidisciplinary discussion and a Gastrografin swallow to understand the patient’s GI anatomy (Figure 3), she underwent a partial gastrectomy, sparing the previous gastric-ileal bypass (Figures 4). The histological examination observed a low-risk GIST (Figure 5), CD117/c-Kit negative, with R0 margins and the mitotic count was 1 mitosis/5 mmq.
The postoperative recovery was free from complications, and the patient began oral feeding without any problems. The hemoglobin value improved (102 g/l), and she was discharged on the 9th postoperative day. The patient was then entrusted to the Oncologists, who, in accordance with the guidelines due to the low-risk profile of the neoplasm, decided not to start adjuvant treatment and preferred a wait-and-watch approach.
A subsequent follow up EGDS, performed one year later, showed well-functioning results of gastroresection on the previous gastric bypass, in the absence of signs of tumor recurrence (Table 1).
Table 1: Bariatric procedures to which the patient has undergone.
| Year |
Bariatric procedures |
| 2004 |
Placement of adjustable gastric banding |
| 2008 |
Removal of adjustable gastric banding |
| 2010 |
Video laparoscopic gastric bypass sec. Amenta-Cariani |
| 2012 |
Gastric bypass revision |
| 2014 |
Resection of the cul de sac of the gastro-jejunum anastomosis, plication of gastric fundus sec. Ramos and jejunal resection at the level of the previous gastro-jejunum anastomosis |
| 2016 |
Adhesiolysis and reduction of common tract, repackaging of E-E anastomosis 60 cm from the ileocecal valve, replication of the gastrojejunal anastomosis, omentectomy |
| 2021 |
Placement of an overstich to repair a gastric-gastric fistula |
| 2021 |
Revision of gastro-jejunum anastomosis and gastric pouch |
Discussion
Obesity is a proven risk factor for many neoplasms. The International Agency for Research on Cancer (IARC) has designated obesity-related cancers, which include hepatocellular carcinoma, exocrine pancreatic cancer, gallbladder cancer, cholangiocarcinoma, colorectal cancer, renal cancer, adenocarcinoma of the esophagus and gastric cardia, prostate cancer, postmenopausal breast cancer, endometrial cancer, ovarian cancer, thyroid cancer, and multiple myeloma [12-15].
There are numerous pathways through which obesity promotes tumorigenesis, including hyperinsulinemia/insulin resistance and abnormalities in Insulin-like Growth Factor-I (IGF-I). Adiposity also influences the synthesis and increased bioavailability of estrogen, androgens, and progesterone, each of which has been linked to cancers through epidemiological studies [16,17]. Chronic inflammation plays a role in cancer as well, as c-Jun NH2-terminal Kinase (JNK) and IκB Kinase-β (IKK-β) are increased in adiposity and may be part of the link between adipose tissue, inflammation, and immune cells involved in cancer formation [17]. Moreover, chronic inflammation contributes to the development of insulin resistance [16,18,19].
Furthermore, both Zhu and Makris have underlined a correlation between ghrelin and GISTs, both of which are mainly located in the fundus of the stomach [20,21]. This may also suggest that GISTs are more frequently observed in patients with obesity than patients without obesity.
On the other hand, Tsui and several other authors have noted a decreased risk of obesity-related and non-related cancer in patients who underwent bariatric surgery. Indeed, Schauer et al. demonstrated that bariatric patients had a 33% lower hazard risk of developing any type of cancer (HR 0.67; 95% CI, 0.6, 0.74; p<0.001) when compared to matched patients with obesity who did not undergo bariatric surgery [22,23]. There are several possible pathways through which bariatric surgery could decrease the risk of cancer in obese individuals. The main one is the improvement of insulin resistance and glucose metabolism, which attenuates metabolic syndrome, decreases inflammation and oxidative stress, improves the regulation of sex hormones, gastrointestinal hormone ghrelin, improves cellular energy homeostasis, and increases energetic efficiency [24].
In the literature, there are very few cases of gastric GISTs after bariatric surgery. In 2006, De Roover reported a case of a 47-year-old woman who presented 12 years after a vertical banded gastroplasty with a gastric pouch outlet obstruction caused by a GIST [25]. In 2019, Musella et al. published a review of literature in which there are 2 cases of GISTs after a sleeve gastrectomy and a laparoscopic Roux-en-Y gastric bypass, respectively [26].
In addition, Parmar et al. conducted a retrospective global study in 2022 on EG malignancies after bariatric surgery and observed that only 3.4% of GISTs occurred in a cohort of 170 patients [27]. In this study, they emphasized that the majority of the cohort consisted of women, with most patients having undergone a Roux-en-Y gastric bypass, followed by adjustable gastric banding and sleeve gastrectomy. The diagnosis of cancer was made 9.5 +/- 7.4 years after bariatric surgery. Despite these findings, they couldn’t establish whether there was an increased risk of EG cancer after bariatric surgery [27].
On the contrary, in 2023, Lazzari et al. conducted a retrospective cohort study involving 908,849 patients with obesity and determined that bariatric surgery was associated with a significant decrease in EG cancer incidence compared to patients who had not undergone bariatric procedures (4.9 vs. 6.9 per 100,000 population per year) [28].
The main point emphasized by the majority of authors is the importance of follow-up. Nevertheless, there is no firm consensus on the timing. A recent consensus statement on sleeve gastrectomy suggested that patients should undergo EGDS every 5 years after sleeve gastrectomy to screen for Barrett’s esophagus [29]. A position statement by the International Federation for the Surgery of Obesity and Metabolic Disorders, on the other hand, suggested that patients should undergo routine endoscopy at 1 year and then every 2-3 years after sleeve gastrectomy and one anastomosis gastric bypass [30].
Conclusion
GISTs are rare neoplasms that can occur in patients underwent bariatric procedures. Diagnosis and management are challenging and require a multidisciplinary approach involving surgeons, gastroenterologists, radiologists, and oncologists. Early detection, accurate diagnosis, and tailored surgical strategies are key elements in achieving favorable outcomes for these patients. With the increasing prevalence of obesity and bariatric surgeries, physicians should remain vigilant in assessing GI symptoms in this specific patient population and should plan for a strict long-term follow-up.
Declarations
Confilict of interest: The authors declare that they have no conflict of interest.
Informed consent: Informed consent to publish potentially identifying information, such as details of the case and images, was obtained from the patient.
References
- Rossi CR, Mocellin S, Mancarelli R et al. Gastrointestinal stromal tumours: From a surgical to a molecular approach. Int J Cancer. 2003; 107: 171–76
- Zhao X, Yue C. Gastrointestinal stromal tumor. J Gastrointest Oncol. 2012; 3: 189–208.
- McDonnell MJ, Punnoose S, Viswanath YKS et al: Gastrointestinal stromal tumours (GISTs): An insight into clinical practice with review of literature. Frontline Gastroenterol. 2017; 8: 19–25.
- WHO Classification of Tumours Editorial Board Soft Tissue and Bone Tumours. 5th ed. IARC, Lyon, France. 2020.
- Agaimy A, Terracciano LM, Dirnhofer S, et al. V600E BRAF mutations are alternative early molecular events in a subset of KIT/PDGFRA wild-type gastrointestinal stromal tumours. J Clin Pathol. 2009; 62: 613–16.
- Soreide K, Sandvik OM, Soreide JA, Giljaca V, Jureckova A, Bulusu VR. Global epidemiology of gastrointestinal stromal tumours (GIST): A systematic review of population-based cohort studies. Cancer Epidemiol. 2016; 40: 39–46.
- Kim JS, Kim HJ, Park SH, Lee JS, Kim AY, Ha HK. Computed tomography features and predictive findings of ruptured gastrointestinal stromal tumors. Eur Radiol. 2017; 27: 2583–2590.
- Kumaresan Sandrasegaran, Arumugam Rajesh, Daniel A Rushing, Jonas Rydberg, Fatih M Akisik, John D Henley. Gastrointestinal stromal tumors: CT and MRI findings. 2005; 15: 1407–1414.
- Papanikolaou IS, Triantafyllou K, Kourikou A, Rösch T. Endoscopic ultrasonography for gastric submucosal lesions. World J Gastrointest Endosc. 2011; 3: 86–94.
- PG Casali, JY Blay, N Abecassis, et al. on behalf of the ESMO Guidelines Committee, EURACAN and GENTURIS. Gastrointestinal stromal tumours: ESMO-EURACAN-GENTURIS Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2021.
- Stroobants S, Goeminne J, Seegers M, et al. 18FDG-positron emission tomography for the early prediction of response in advanced soft tissue sarcoma treated with imatinib mesylate (Glivec). Eur J Cancer. 2003; 39: 2012-2020.
- Wolin KY, Carson K, Colditz GA. Obesity and cancer. Oncologist. 2010; 15: 556-65.
- Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med. 382 2003; 348: 1625-38.
- Calle EE, Thun MJ. Obesity and cancer. Oncogene. 2004; 23: 6365-78.
- Bianchini F, Kaaks R, Vainio H. Overweight, obesity, and cancer risk. Lancet Oncol. 2002; 3: 565-74.
- Calle EE, Kaaks R. Overweight, obesity and cancer: epidemiological evidence and proposed mechanisms. Nat Rev Cancer. 2004; 4: 579-91.
- Roberts DL, Dive C, Renehan AG. Biological mechanisms linking obesity and cancer risk: new perspectives. Annu Rev Med. 2010; 61: 301-16.
- Kahn BB, Flier JS. Obesity and insulin resistance. J Clin Invest. 2000; 106: 473-81.
- Erlinger TP, Platz EA, Rifai N, Helzlsouer KJ. C-reactive protein and the risk of incident colorectal cancer. JAMA. 2004; 291: 585-90.
- Zhu CZ, Liu D, Kang WM, Yu JC, Ma ZQ, Ye X, et al. Ghrelin and gastrointestinal stromal tumors. World J Gastroenterol. 2017; 23: 1758–1763.
- Makris MC, Alexandrou A, Papatsoutsos EG, Malietzis G, Tsilimigras DI, Guerron AD, et al. Ghrelin and obesity: Identifying gaps and dispelling myths. A Reappraisal. In Vivo. 2017; 31: 1047–1050.
- Tsui ST, Yang J, Zhang X, Docimo Jr. S, Spaniolas K, Talamini M, Sasson AR, Pryor AD, Development of Cancer after Bariatric Surgery, Surgery for Obesity and Related Diseases. 2020.
- Schauer DP, Feigelson HS, Koebnick C, Caan B, Weinmann S, Leonard AC, et al. Bariatric Surgery and the Risk of Cancer in a Large Multisite Cohort. Ann Surg. 2019; 269: 95-101.
- Ashrafian H, Ahmed K, Rowland SP, Patel VM, Gooderham NJ, Holmes E, et al. Metabolic surgery and cancer: protective effects of bariatric procedures. Cancer. 2011; 117: 1788-1799.
- De Roover A, Detry O, De Leval L, Coimbra C, Desaive C, Honoré P, Meurisse M Report of two cases of gastric cancer after bariatric surgery: lymphoma of the bypassed stomach after Roux-en-Y gastric bypass and gastrointestinal stromal tumor (GIST) after vertical banded gastroplasty Obes Surg. 2006; 16: 928-31.
- Musella M, Berardi G, Bocchetti A, Green R, Cantoni V, Velotti N, Di Lauro K, Manzolillo D, Vitiello A, Milone M, De Palma G D Esophagogastric Neoplasms Following Bariatric Surgery: an Updated Systematic Review Obes Surg. 2019; 29: 2660-2669.
- Parmar C, Zakeri R, Abouelazayem M, Shin T H, Aminian A, Mahmoud T, et al. OGMOS Study Group Esophageal and gastric malignancies after bariatric surgery: a retrospective global study Surg Obes Relat Dis. 2022; 18: 464-472.
- Lazzati A, Poghosyan T, Touati M, Collet D, Gronnier C Risk of Esophageal and Gastric Cancer After Bariatric Surgery JAMA Surg. 2023; 158: 264-271.
- Mahawar KK, Omar I, Singhal R, et al. The first modified Delphi consensus statement on sleeve gastrectomy. Surg Endosc. 2021; 35: 7027–33.
- BrownWA, Johari Halim Shah Y, Balalis G, et al. IFSO position statement on the role of esophago-gastro-duodenal endoscopy prior to and after bariatric and metabolic surgery procedures. Obes Surg. 2020; 30: 3135–53.