Introduction
Stress cardiomyopathy is a temporary condition that mimics acute myocardial infarction. It is also known as Takotsubo cardiomyopathy, apical ballooning, octopus heart syndrome, or broken heart syndrome [1]. A stressful event often triggers this reversible cardiomyopathy and presents similarly to myocardial infarction. It has been most commonly reported in postmenopausal women, with emotional or physical stress frequently identified as the triggering factor [2].
Takotsubo cardiomyopathy was first described by Dote et al. in Japan in 1991. The name derives from the shape of the left ventricle seen on ventriculography, which resembles the octopus-catching vessel used by Japanese fishermen [1].
Case reports
Case-1
A 42-year-old frail-looking female patient with ovarian carcinoma, who had no other comorbidities, completed 6 cycles of chemotherapy (paclitaxel and carboplatin) and was scheduled for cytoreductive surgery. The procedure was done under general anesthesia with an epidural catheter insertion. During the surgery, the patient had a blood loss of approximately one liter and received 2-litres crystalloid, two units of Packed Red Blood cells (PRBCs). Due to the significant blood loss and the need for vasopressors, she was transferred to the ICU and placed on mechanical ventilation with sedation. The patient received one more unit of PRBC in the ICU.
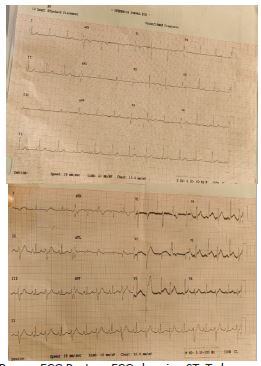
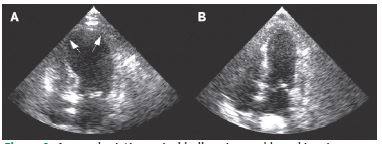
During the preoperative evaluation, the ECG and 2D echocardiogram were normal (Figure 1). However, the patient’s condition later deteriorated with an increased dose of noradrenaline and vasopressor support, and a Point-of-Care Ultrasound (POCUS) examination revealed hypokinesia in both the apical and mid-regions of the heart, along with apical ballooning, indicating left ventricular dysfunction (Figure 2). A cardiologist subsequently confirmed these findings. The blood gas analysis showed metabolic acidosis with a lactate 3 mmol/lt. Further investigations are shown in Table 1.
In the postoperative period, the high-sensitivity troponin I level was 779.9 ng/L, well above the normal upper limit of 19 ng/L. Chest X-ray appears normal as shown in (Figure 3).
The cardiologist recommended coronary angiography; however, due to the high risk of post-operative bleeding and the need for anticoagulants, a discussion with the surgeon led to deferring the angiography. Meanwhile, the patient received supportive care, and the need for vasopressors decreased. By postoperative day 2, the patient was extubated and transferred to the ward.
Three weeks after discharge, a follow-up with a 2D echocardiogram showed no abnormalities. Ventricular wall motion and contractility were returned to normal.
Case-2
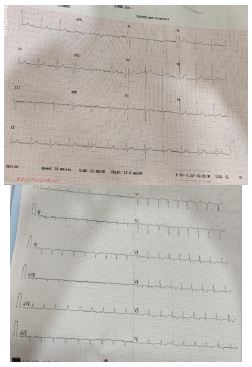
A 62-year-old postmenopausal woman with normal ECG (Figure 4) and ECHO, a k/c/o buccal mucosa carcinoma underwent a composite resection and fibular free flap under general anesthesia. The surgery was uneventful, but due to its prolonged duration and shared airway, she was put on the mechanical ventilator.
In the ICU, the patient had a sudden hypotension and bradycardia, becoming pulseless. CPR was started according to ACLS protocols, and after two minutes, circulation was restored. However, she still had hypotension and noradrenaline and vasopressin requirements.
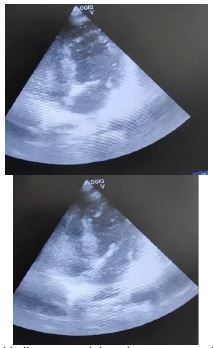
Arterial blood gas analysis revealed metabolic acidosis with elevated lactate levels. A bedside POCUS (Point-of-Care UltraSound) was performed, which showed apical ballooning and apical hypokinesia, indicating left ventricular dysfunction with an ejection fraction of 40%, later confirmed by the cardiologist (Figure 5).
A high-sensitive troponin I level was measured at 913.7 ng/l, indicating cardiac injury, well above baseline 19 ng/l. Lab values are shown in Table 2.
Chest X-ray on the postoperative day is shown in Figure 6.
The cardiologist recommended coronary angiography; however, later postponed i/v/o hemodynamic instability. Gradually the patient’s need for vasopressors decreased, and blood acidosis resolved. The patient was extubated on postoperative day 2 and discharged on day 7 with follow-up instructions. A follow-up echocardiogram four weeks later showed normal ventricular contractility and no motion abnormalities.
Table 1: Investigations of case 1.
| Hb/tlc/plt |
11.9/16.42/162 |
13.8/15.03/155 |
11.3/11.43/150 |
| Urea/creat |
26.8/0.54 |
35.6/0.63 |
44.7/0.62 |
| Na/k |
136.8/3.69 |
134.7/3.78 |
132/3.39 |
| INR |
1.647 |
|
|
Table 2: Lab values of case 2.
| Hb/tlc/plt |
10.6/21.81/294 |
11.8/19.07/217 |
| Urea/creat |
18/0.51 |
29.1/0.61 |
| Na/k |
133.4/4.09 |
137.3/3.93 |
| INR |
1.33 |
|
Discussion
Mayo criteria for diagnosing stress cardiomyopathy or Takotsubo cardiomyopathy [4].
⮚ Transient hypokinesis, akinesis/dyskinesis of the left ventricular mid segments, with or without apical involvement.
⮚ Absence of obstructive coronary disease.
⮚ New ECG abnormalities -> ST elevation/T inversion or modest increase in troponin.
⮚ Absence of pheochromocytoma and myocarditis.
Stress cardiomyopathy is usually triggered by internal or external sources of stress. In patients affected by this condition, plasma catecholamine levels are two to three times higher than those observed in individuals with myocardial infarction, indicating that elevated catecholamines play a crucial role in this disorder [5].
Increased catecholamines may alter intracellular signaling, negatively impacting heart function leads to transient and reversible Left Ventricular (LV) dysfunction, particularly at the apex of the myocardium. Additionally, patients may have pre-existing endothelial dysfunction and reduced coronary artery reserve, making them more susceptible to stress cardiomyopathy during acute stress [2]. This condition primarily affects women, representing about 90% of cases, though the reasons are unclear. Hessel estimated that stress cardiomyopathy occurs in approximately 1 in 6,700 cases, with 37% of cases reported during anesthesia or surgery [6].
In our patient, the factors that may have contributed to an increased catecholaminergic state and subsequent TTC include: (1) stress of the procedure and (2) inadequate depth of anesthesia, (3) pre-existing conditions contributing to stress cardiomyopathy (4) exposure to exogenous catecholamines through injection of local anesthetic mixed with epinephrine before starting the procedure. Other contributing factors include the patient’s gender and the history of autoimmune disease, which could precipitate endothelial dysfunction. Various case reports of stress cardiomyopathy have been documented post-surgery.
Similar to our case, Nath MP et al. [7] L. Meng et al. [8] Ruth Bird et al. [10] Bogdan Moldovan et al. [3] reported cases of post-operative stress cardiomyopathy and managed them conservatively.
Case reports have shown that bedside Transthoracic Echocardiography (TTE) can be instrumental in the rapid diagnosis of Takotsubo cardiomyopathy, helping to reduce the significant morbidity associated with the condition. It is important to note that both stress cardiomyopathy and acute coronary syndrome can present with similar symptoms and elevated cardiac enzyme levels. Thus, echocardiography and angiography can be invaluable in distinguishing between regional wall motion abnormalities that suggest a vascular origin and stress cardiomyopathy.
Conclusion
Stress cardiomyopathy can occur in the perioperative setting due to pre-existing conditions, inadequate depth of anesthesia, and intraoperative epinephrine administration leading to catecholamine surge contributing to stress cardiomyopathy. A high index of suspicion for stress cardiomyopathy must be present for patients who have a cardiac arrest with potential precipitating conditions, such as female gender, stress of the event, and preexisting autoimmune conditions. Supportive therapy is key in the management of stress cardiomyopathy.
Declarations
Conflict of interest: The authors declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Patient consent statement: We hereby confirm that we have obtained written informed consent from the patient in this case report for publication of their clinical information.
Funding: The authors did not receive any financial support for the research, authorship, or publication of this article.
Authors contributions: All authors read and agreed to the published version of the manuscript.
References
- Dote K, Sato H, Tateishi H, Uchida T, Ishihara M. Myocardial stunning due to simultaneous multivessel coronary spasms: a review of 5 cases. J Cardiol. 1991; 21: 203–214.
- Jothin A, Raj JP, Thiruvenkatarajan V. A simple procedure in a complex patient: perioperative takotsubo cardiomyopathy. BMJ Case Rep. 2020; 13: e233121.
- Moldovan B, et al. Takotsubo Cardiomyopathy After Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for a Recurrent Colon Cancer: A Life-Threatening Complication. Diagnostics. 2024; 14: 2402.
- Medina de CH, et al. Stress Cardiomyopathy Diagnosis and Treatment. J Am Coll Cardiol. 2018; 72: 1955–1971.
- Park JT, et al. Stress-induced cardiomyopathy after general anesthesia for total gastrectomy -A case report-. Korean J Anesthesiol. 2010; 58: 299–303.
- Hessel EA. Takotsubo cardiomyopathy and its relevance to anesthesiology: a narrative review. Can J Anaesth. J Can Anesth. 2016; 63: 1059–1074.
- Post-Operative Takotsubo Cardiomyopathy: Case Report and Review of Literature: How Much we Know. J Anesth Crit Care Open Access. 2016: 4.
- Meng L, Wells C. Takotsubo Cardiomyopathy during Emergence from General Anaesthesia. Anaesth Intensive Care. 2009; 37: 836–839.
- Mihalcea L, Sebastian I, Simion-Cotorogea M, Klimko A, Droc G. Reverse Takotsubo Cardiomyopathy after Orthotopic Liver Transplantation. A Case Report. J Crit Care Med Univ Med Si Farm Din Targu-Mures. 2022; 8: 117–122.
- Bird R, Saleh A, Riley T, Smith H, Dempsey C. Takotsubo Cardiomyopathy Post Induction of Anesthesia. J Med Cases. 2015; 6: 437–439.