Introduction
Tuberculosis is an infectious disease caused by mycobacterium tuberculosis, an acid-alcohol-resistant bacilli. It is transmitted by inhalation of aerosols exhaled by a person with active pulmonary or laryngeal tuberculosis. It is estimated that only 10% of persons infected with Mycobacterium tuberculosis will develop a clinical manifestation of the disease [1].
Pulmonary tuberculosis is the most common clinical manifestation, however, other systems such as the nervous, digestive and cardiovascular systems may also be affected. When the disease presents in a cardiovascular form, pericarditis associated with pericardial effusion is the most important manifestation, occurring in approximately 5% of immunocompetent patients [2].
Tuberculosis is the leading cause of pericardial effusion in sub-Saharan african countries particularly Cameroon. In Africa, tuberculosis represent 79% of etiology of adults pericardial effusion, 15% of effusive constrictive and a large proportion of them (up to 20%) responsible of cardiac tamponade [1] .
The subxiphoid Surgical drainage is the procedure of choice in the treatment and prevention of cardiac tamponade due to abundant tuberculous pericardial effusion [3] . Few studies have been published about surgical drainage of tuberculous pericardial effusion despite of the high prevalence of tuberculosis in Cameroon. The aim of this case report shows the effectiveness and safety of the subxiphoid surgical management of tuberculous pericardial effusion.
Case presentation
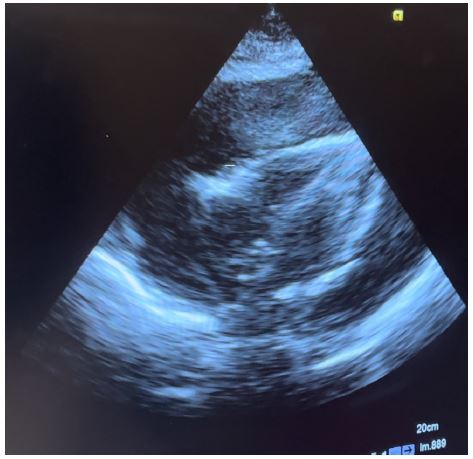
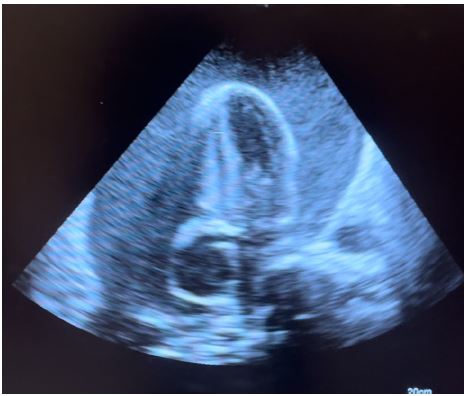
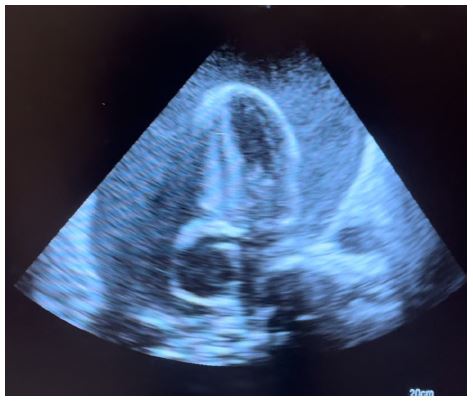
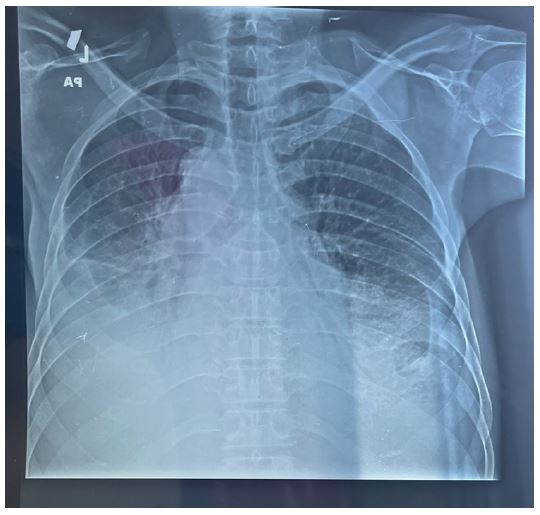
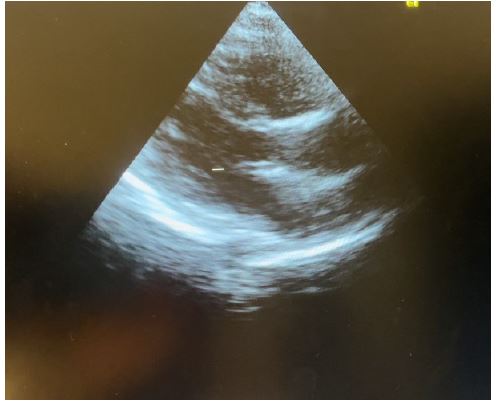
Presenting a 50-year-old immunosuppressed patient who was referred to our hospital for management of massive pre-tamponade pericardial effusion in respiratory distress. Patient was received in the emergency department and an emergency cardiac echography was done which confirmed the referral diagnosis of massive pre-tamponade pericardial effusion with massive bilateral pleural effusions. Patient was immediately prepared and taken for subxiphoid surgical drainage.
Surgical procedure
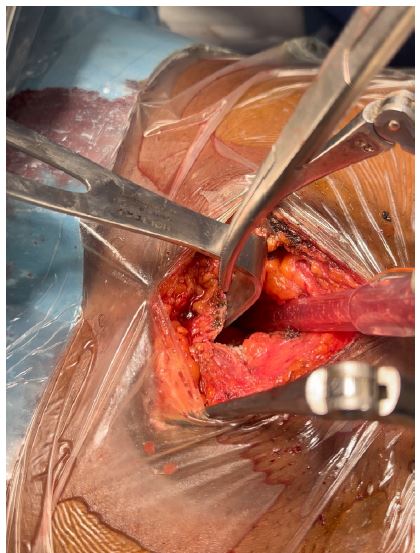
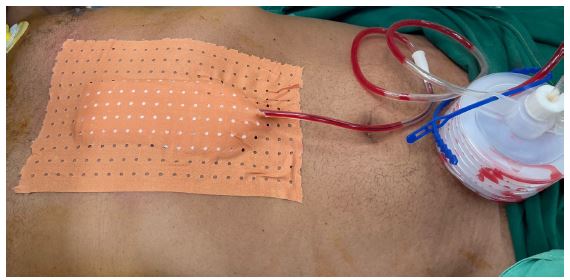
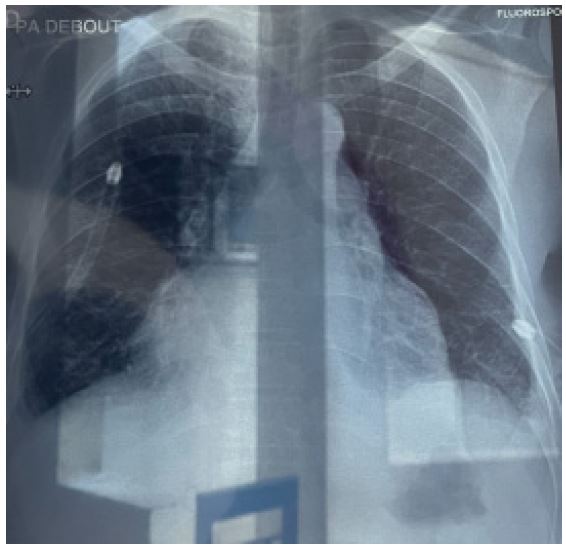
Patient was placed under general anesthesia, intubated and placed in the supine position on the surgical bed. Routing disinfection and surgical prepping was done. A subxiphoid median incision starting from xiphoid process to about 7 cm inferiorly was made. Subcutaneous and muscle fascia dissected and the xiphoid process amputated for better exposure of the pericardium. The bulging pericardium seen with a pericardiotomy made gently on the pericardium. Approximately 2 Liters of serohematic pericardial fluid was drained and a pericardial drain was placed in the pericardial space and connected to a self-expanding vacuum drain which was intended to drain the rest of the pericardial fluid. A biopsy of the pericardium was collected alongside 10cc of pericardial fluid and send for histo-cytology studies to determine the etiology of the effusion. Two thoracic drains were also placed and suture wounds closed up according to standard fashion and patient was taken to the surgical ward afterwards. Post operatively, cardiologist and infectious disease consults were requested for the patient. Post operative follow up was done. Histo-cytology results confirming TB as the etiology of the effusion. Patient was placed on anti TB medimedications by the infectious disease doctor and patient improved clinically and symptomatically with drained not producing anymore. Patient was later discharged 10 days post operatively and reviewed 2 weeks after with follow up cardiac echo and chest Xray not showing any pericardial effusion and pleural effusion respectively.
Discussion
Acute pericarditis presents the most common manifestation of pericardial disease and accounts for about to 5% of patients admitted to the emergency department with chest pain not due to myocardial infarction. Viral and idiopathic causes presents the most prevalent etiologies; however, several conditions can cause an acute pericardial inflammation such as autoimmune diseases, uremia, and bacterial infections [6].
Some common pathogens include Staphylococcus, Streptococcus, Haemophilis and Mycobaterium tuberculosis [3].
Despite the fact that effective treatments exist, tuberculosis remains a public health problem, especially in developing countries. In 2017, there were about 10 million estimated new cases and 1.6 million deaths from tuberculosis globally [4]. Pericardial involvement caused by mycobacterium tuberculosis, is common in immunosuppressed patients [2].
Physical examination is important in making the diagnosis of pericardial effusion. Massive pericardial effusion leads to tamponade [17]. Therefore, clinician must find quickly all signs of tamponade in patients admitted for pericardial effusion.
According to one study, the commonest signs of pericardial effusion were tachycardia (95%), jugular venous distension (56%) and muffled heart sounds (56%). Beck’s triad is a collection of three clinical signs associated with pericardial tamponade which is due to an excessive accumulation of fluid in pericardial sac. The Beck’s triade associate low blood pressure, muffled heart sounds and raised jugular venous pressure.
There was 20% of pericardial tamponade among 10 patients presented pericardial effusion due tuberculosis in study of Yaméogo et al. performed in Burkina Faso [18].
Electrocardiogram is one of non-invasive test, used to detect the signs of massive pericardial effusion or tamponade pericarditis. In massive pericardial effusion with cardiac tamponade, ECG found classical triad of sinus tachycardia, low QRS voltages and electrical alternans [17]. Kombila et al. found 62% of low QRS voltages in patients with tuberculous pericardial effusion in Libreville [7].
Transthoracic echocardiography is the best diagnostic imaging, useful in diagnosis and management of tuberculous pericardial effusion. Echocardiography can provide an estimate of the size of effusions. Generally, the size of the effusion on echocardiography indicates the volume of pericardial fluid as follows: small (<10 mm), which corresponds to 50-100 mL pericardial fluid; moderate (10-20 mm), corresponding to 100 - 500 mL pericardial fluid and large (>20 mm), corresponding to >500 mL pericardial fluid [19] . The study of Diakité et al. showed 18% of moderate abundance and 81% of high abundance among 49 cases of tuberculous pericarditis [6].
The definitive diagnosis of tuberculous pericardial effusion requires sometimes differents tests. Cytology and biochemical tests of pericardial fluid are usually not enough to establish the diagnosis of tuberculous pericardial effusion. Histopathology of pericardial biopsies from pericardial window are important to make definitive diagnosis of tuberculosis in pericardial effusion [20]. Histological features of granulomatous inflammation and caseous necrosis are highly suggestive of tuberculosis.
GeneXpert is a rapid, sensitive and specific diagnostic tool to detect Mycobacterium tuberculosis in pericardial effusion. The pooled sensitivity, specificity of Xpert MTB/RIF for tuberculous pericarditis were 65% and 99% [21].
Pericardial drainage is indicated in patients with cardiac tamponade. Constrictive pericarditis is the most important complication of tuberculous pericarditis and occurs in 30% to 60% of cases. Pericardiectomy is recommended if the patient does not respond satisfactorily after four to eight weeks of antituberculous treatment [11].
Mortality rate of tuberculous pericardial effusion was higher in sub-Saharan african countries than western countries. The rarity of cardiac surgeon and the delay of diagnosis contribute to high mortality rate in these countries. The overall mortality rate in patients treated for tuberculous pericarditis was 26% in sub-Saharan african countries [4].
Conclusion
Subxiphoid surgical drainage is a more effective and trustworthy method; it is thought that this method is more effective in diagnosis and treatment as it allows biopsy, examination and removal of the adhesions within the pericardial space.
References
- Rajaobelison, T. , Randimbinirina, Z. , Ramifehiarivo, M. , Rabarison, M. , Rajaonanahary, T. and Rakotoarisoa, A. (2024) Subxyphoid Pericardial Drainage for Tuberculous Pericardial Effusion in Antananarivo. World Journal of Cardiovascular Surgery. 14: 21-31.
- Becit N, Unlü Y, Ceviz M, Koçogullari CU, Koçak H, Gürlertop Y. Subxiphoid pericardiostomy in the management of pericardial effusions: case series analysis of 368 patients. Heart. 2005; 91(6): 785-90.
- Colak A, Becit N, Kaya U, Ceviz M, Kocak H. Treatment of Pericardial Effusion Through Subxiphoid Tube Pericardiostomy and Computerized Tomography- or Echocardiography - Guided Percutaneous Catheter Drainage Methods. Braz J Cardiovasc Surg. 2019; 34(2): 194-202.
- Snyder, Matthew J., Jennifer Bepko, and Merima White. “Acute pericarditis: diagnosis and management.” American family physician. 2014; 89(7): 553-560.
- Noubiap, J.J., Agbor, V.N., Ndoadoumgue, A.L., Nkeck, J.R., Kamguia, A., Nyaga, U.F., et al. (2019) Epidemiology of Pericardial Diseases in Africa: A Systematic Scoping Review. Heart. 105: 180-188.
- Noubiap, J.J., Agbor, V.N., Ndoadoumgue, A.L., Nkeck, J.R., Kamguia, A., Nyaga, U.F., et al. (2019) Epidemiology of Pericardial Diseases in Africa: A Systematic Scoping Review. Heart. 105: 180-188.