Background
Colorectal cancer is one of the most common cancers worldwide. The prognosis has improved over the years due to national screening programmes, the development of diagnostic tools and multidisciplinary therapeutic approaches that are individually tailored [1-4]. However, the treatment of advanced stages of cancer with distant metastases remains challenging [5].
The lungs and liver are the most frequent sites of metachronous colorectal cancer metastases. Less frequently, peritoneal metastases or ovarian metastases appear in women, and only occasional reports mention the spleen, thyroid gland, urinary tract, adrenal gland, stomach, skeletal muscle, and abdominal wall as recurrence sites [6].
However, isolated metachronous metastases of colorectal cancer sequentially appearing in one patient in the ovary, gastric wall, and abdominal wall are extremely rare and have never been reported in the medical literature.
The main aim of this article is to evaluate published literature regarding to the role of surgery in unusual locations of metastases from CRC, specifically ovarian, gastric, and abdominal wall sites.
Case presentation
A 43-year-old female was admitted to the Department of General Surgery at a district hospital suffering from severe abdominal pain, vomiting and fatigue in December 2013. The patient was otherwise fit and well and did not report any weight loss or change of bowel habits. The patient had no prior history of any medical or surgical illnesses, was not on any medication, and had no family history of cancer.
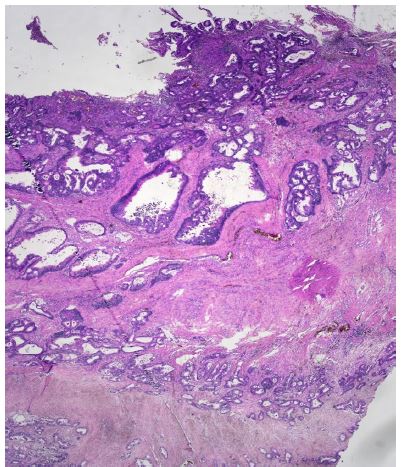
An abdominal Computed Tomography (CT) scan discovered a dilated colon up to the splenic flexure. A CT scan did not show regional nor distant metastases. Subsequently, the patient underwent exploratory laparotomy, which showed an obstructive tumour in the middle of the transverse colon, and there were no signs of macroscopic metastases in the abdominal cavity. The patient underwent resection of the transverse colon with end-to-end anastomosis. Postoperatively, the patient recovered well. Histopathological examination of the specimen revealed a moderately differentiated tubar adenocarcinoma, irregularly infiltrating the serosa, without lymphovascular invasion (Figure 1a), (T4a) and without nodal involvement (11 negative pericolic and 1 negative mesenteric lymph nodes were found); pT4a, N0, M0 (stage IIA); R0 resection was performed. Microsatellite instability-high (MSI-H) cancer was not proven.
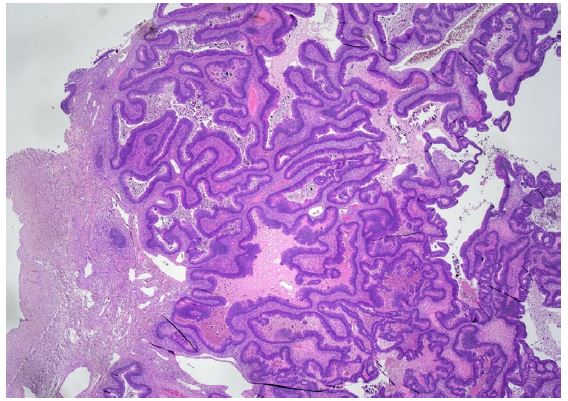
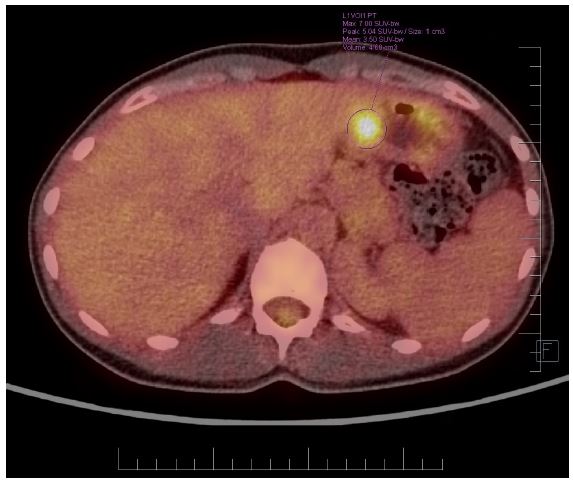
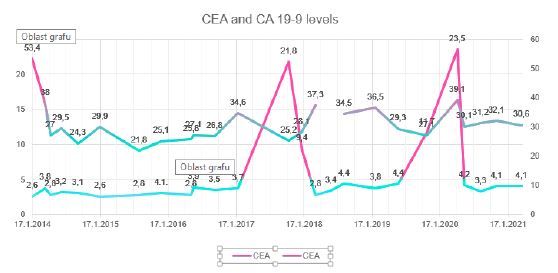
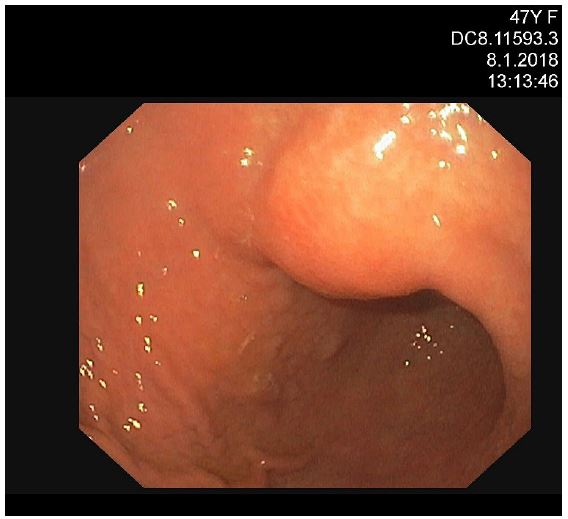
Nevertheless, the patient was assessed by a colorectal Multidisciplinary Team (MDT) at Masaryk Memorial Cancer Institute (MMCI), which decided on adjuvant therapy for the stenotic tumour. Adjuvant chemotherapy on the base of 5 fluorouracil (FU/FA Mayo) was administered. However, this was converted to monotherapy capecitabine due to an allergic skin reaction and neutropenia grade IV. Further therapy was uncomplicated, and close follow-up was recommended. An elevation of tumour marker Carcinoembryonic Antigen (CEA) of 21,8 μg/l was found in October 2017. However, a normal level of the Carbohydrate Antigen (CA) 19-9 of 25.2 ng/ml was noted. Subsequent assessment revealed a left ovarian mass with suspicion of a metastatic process. In November 2017, the patient underwent a gynaecologic evaluation followed by explorative laparotomy at the Department of Gynaecology in the University Hospital Brno. A hysterectomy with bilateral oophorectomy and appendectomy was performed, and malignant ascites was also found. Histological findings showed metastases of moderately differentiated intestinal adenocarcinoma in the left ovary (Figure 1b), identical to the primary transverse colon tumour resected in 2013. KRAS, NRAS and BRAF gene mutations were not detected. The postoperative recovery was uncomplicated, and the patient was referred back to medical oncologists at MMCI. A follow-up Positron Emission Tomography/Computed Tomography (PET/CT) scan was performed in December 2017. It discovered a small metabolically active lesion measuring 12 mm located in the pyloric region closer to the gastric, small curvature (Figure 2). Tumour marker CEA was again slightly elevated (9,4 μg/l) (Figure 3). A gastroduodenoscopy showed prominent gastric walls in the region of the angular notch without mucosal changes. A biopsy was taken, and histologic examination revealed benign atrophic gastritis only (Figure 4).
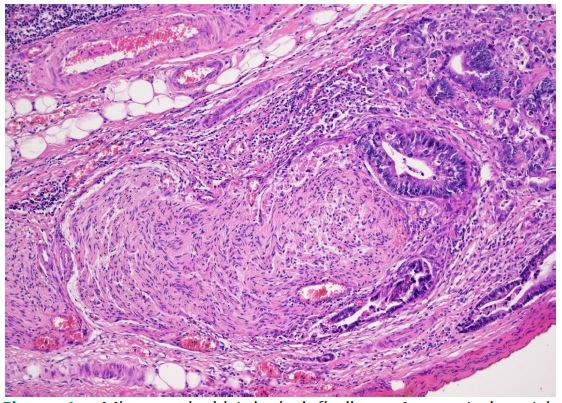
However, based on the results of PET/CT, tumour marker elevation, malignant ascites, previous results and the course of the disease, the case was discussed at the colorectal MDT in the MMCI. The MDT recommended explorative laparotomy. In February 2018, surgery was performed with findings of a gastric lesion and multiple peritoneal metastases. Gastric resection in Billroth I modification with small and great curvature lymphadenectomy and omentectomy was performed, followed by cytoreductive surgery, resection of the peritoneum, and HIPEC for 90 minutes with cisplatin and mitomycin using Rand’s Performer HT device (Medolla, Italy). The postoperative recovery was uncomplicated, and the patient was discharged on the eleventh postoperative day. Histologic examination found metastases of moderately differentiated adenocarcinoma of colorectal origin with perineural invasion in the gastric antrum wall without mucosal changes (Figure 1c). Six lymphatic perigastric and five omental lymph nodes were harvested, and all nodes and peritoneal strips were negative for cancer. Adjuvant chemotherapy based on capecitabine and oxaliplatin (XELOX) was administered and the patient was followed in four-month intervals.
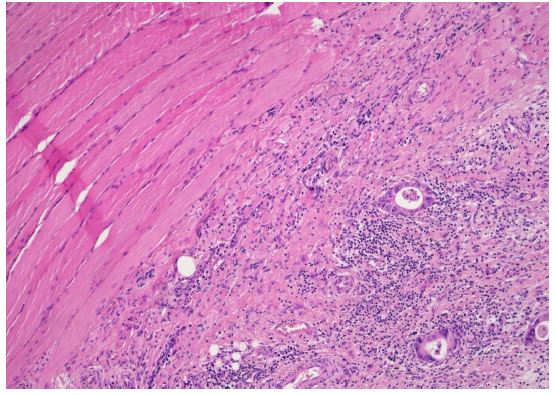
Further elevation of serum tumour markers - CEA and CA 19-9 - was noticed in March 2020. The CT scan of the thorax and abdomen revealed a small lesion in the abdominal wall, measuring approximately 3 cm in diameter. No additional pathology was identified on the CT scan. The colorectal MDT recommended surgical resection of the suspicious abdominal wall lesion with reconstruction of the abdominal wall. The surgery was performed on 29 April 2020. The abdominal wall was resected in full thickness and substituted with Vicryl and Prolene meshes. No signs of pathology in the abdominal cavity were found. The patient was discharged on the fifth postoperative day. Histopathologic examination of the specimen revealed metastatic adenocarcinoma of colorectal origin (Figure 1d), and R0 resection was performed. Medical oncologists suggested follow-up without any adjuvant treatment, and the patient agreed. In January 2025, the patient returned to our clinic for a follow-up. The patient was fit and well without any signs of cancer recurrence.
Discussion and conclusions
Due to better diagnostic tools, the use of modalities, such as CT scan, MRI, or PET/CT, PET/MRI, coupled with the increasing survival of cancer patients, repeat metastases are more likely to be diagnosed. The clinical outcomes of patients with colorectal metastases differ significantly depending on a wide range of factors, including the choice and the timing of treatment. Palliative chemotherapy without curative intent is considered as the golden standard for metastatic colorectal cancer. Nevertheless, there is a clear benefit of radical surgery compared to systemic therapy alone. A surgical resection of metastases from colorectal cancer remains significant, aiming to extend patient long-term survival or even cure selected patients. However, only limited data is available to evaluate the role of radical surgery for repeatedly distant metastases in less frequent anatomical sites.
Several clinicopathological factors predict a patient’s survival after repeat resection: the status of the primary colorectal cancer, the interval between colorectal and recurrence, the number of lesions, the size of metastases, parenchymal involvement and the total tumour volume of metastasis, and the preoperative serum CEA level [6].
The 5-year survival rate of patients who have undergone hepatic resection of metastases from colorectal cancer has been reported to vary from 25% to 40% [6,7]. In colorectal cancer, the most prevalent form of recurrence was in the liver remnants (41.4%), followed by a recurrence of pulmonary metastasis (19.2%) and others (7.2%) [8]. A repeated metastasectomy of liver or pulmonary metastasis for repeat distant recurrence from colorectal cancer is now widely accepted to provide good results for selected patients. However, using this approach for metastases in unusual anatomical sites was only suggested in a few retrospective studies, with some long-term survival reports [9].
In 2020, Colloca et al. identified 425 patients with distant metastases of colorectal cancer, and they reported that the survival after a metastasis diagnosis was shorter in the synchronous group (18.5 vs. 62.8 months, p<0.001) [10]. Most reports consider synchronous liver metastases from CRC to be more aggressive than metachronous [11,12]. However, patients with metachronous colorectal cancer metastases other than liver or pulmonary are extremely rare. So far, we have found only one case report of metachronous colorectal cancer metastases to unusual extrahepatic sites, the stomach and abdominal wall, in the literature [13].
The incidence rate of ovarian metastases from colorectal cancer is between 3 and 10% and is linked to a more unfavourable prognosis [14]. Usually, the patient reports symptoms such as abdominal pain or abdominal distension. In 2009, Kim et al. published a Korean study that evaluated 103 patients with metastatic colorectal cancer to the ovary. The 5-year DFS was 26,6% and OS 40.1%. Multivariate analysis identified extra-ovarian metastases (50.9% versus 15.6%, p=0.0035) and bilateral ovarian metastases (36.4% versus 10.6%, p=0.015) as poor prognostic factors. Additionally, other retrospective studies suggest a lower response to chemotherapy in ovarian metastases when compared to other metastatic sites. In 1995, authors from the Royal Marsden Hospital, London, published a study with 51 patients. The response rate to chemotherapy was 31% for extra ovarian metastasis and 14% for ovarian metastases, suggesting that ovaries may act as metastatic sanctuaries for colorectal cancer [15]. Therefore, surgery in patients with symptomatic disease seems more appealing since chemotherapy does not induce a reasonable response rate. Radical resection (R0) should always be the main purpose, aiming to increase a patient’s long-term survival.
Peritoneal metastases associated with colorectal cancer are considered a very poor prognostic condition. In the late 1980s, Sugarbaker developed a Cytoreductive Surgery method (CRS) combined with Hyperthermic Intraperitoneal Chemotherapy (HIPEC). HIPEC and CRS have gained popularity in the last decades as an aggressive treatment option, intending to either extend Disease-Free Survival (DFS) or cure selected patients with peritoneal metastases [16,17]. In 2007, Sugarbaker reported study results which estimated a 5-year OS for patients undergoing CRS with HIPEC ranges from 11 to 32%. Additionally, some retrospective studies observed a cure rate (DFS longer than 5 years) of 16-22% following CRS and HIPEC. Between 1998 and 2001, Verwaal in the Netherlands randomly assigned 105 patients to either HIPEC with CRS or systemic therapy with 5-Fluorouracil (5-FU), with or without palliative surgery. Median OS was superior in the CRS arm, 22.3 months versus 12.6 months for systemic chemotherapy (p=0.032) [18].
Gastric metastasis from CRC is rare. In 2001, Oda et al. published a cohort of 347 autopsies of patients with colorectal cancer in which 5.4% had occult gastric metastases, and half of all gastric metastases were mimicking submucosal tumours [19]. The most common primary tumours, which tend to spread to the stomach, were metastases in the lung, breast, malignant melanoma and oesophagus. Typical endoscopic features of gastric metastasis include submucosal and polypoid lesions with central depression [20]. While our case also showed that the endoscopic appearance resembled a submucosal tumour accompanied by central depression and erosion, CRC as a primary site is extremely unlikely, as the biopsy showed chronic gastritis only.
Additionally, our study has potential limitations, such as selection bias, which means the study focuses only on patients with favourable conditions (e.g., good performance status, isolated metastasis sites, and longer disease-free intervals). This could limit generalizability to broader patient populations. There is also an absence of control groups, as there is no comparison with patients who did not undergo repeat metastasectomy or received alternative treatments. In addition, there are potential confounding factors, for the reason that the study may not adequately address other factors influencing long-term survival, such as genetic predispositions, other concurrent treatments, or overall healthcare access. Finally, the study inherently focuses on a patient who survived, potentially overlooking cases where repeat metastasectomy was unsuccessful.
In conclusion, a careful selection of patients indicated for surgery plays a key role in improving long-term survival. Potential features suggesting a greater benefit from metastasectomy are an isolated metastasis site, a longer disease-free interval from previous treatment, complete resectability, and the patient’s good performance status. As of January 2025, our patient is in very good overall condition without any signs of relapsed disease. With an Overall Survival (OS) exceeding 11 years, our patient demonstrates one of the most favourable survival outcomes among those reported in published case studies involving repeat metastasectomy [21]. For that reason, repeat resection of metachronous metastases, which some would consider as an aggressive radical surgery, followed by subsequent tailored systemic treatment, can be the treatment of choice. This might significantly prolong survival in carefully selected patients. It appears that aggressive radical surgical resection and further tailored systemic treatment can be the treatment of choice even for repeatedly recurring diseases in unusual locations [6].
Author declarations
Ethics declarations and consent for publication: As per the Masaryk Memorial Cancer Institute Institutional Review Board, case reports do not need ethical approval or patient consent as long as there is no intervention and no patient identifiers appear in the report. Therefore, neither ethical approval nor patient consent was required for this case report; however, written informed consent was obtained from the patient involved in this study for the publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Availability of data and materials: The data are not publicly available due to the data being confidential patient data but are available from the corresponding author on reasonable request.
Competing interests: The authors declare that they have no competing interests.
Funding: This work was supported by MH CZ – DRO (MMCI, 00209805).
Author’s contributions: study design, drafting of the manuscript; PK: study design, draft of the manuscript; LN and JT: participated in the design of the study; LF, JN and AH: data collection and editing; VJ: supervision and critical review.
All authors read and approved the final manuscript.
References
- Horn SR, Stoltzfus KC, Lehrer EJ, Dawson LA, Tchelebi L, et al. Epidemiology of liver metastases. Cancer Epidemiol. 2020; 67: 101760.
- Dal Maso L, Panato C, Guzzinati S, Serraino D, Francisci S, et al. Prognosis and cure of long-term cancer survivors: A population-based estimation. Cancer Med. 2019; 8: 4497-4507.
- Arnold M, Sierra MS, Laversanne M, Soerjomataram I, Jemal A, et al. Global patterns and trends in colorectal cancer incidence and mortality. Gut. 2017; 66: 683-691.
- Dekker E, Tanis PJ, Vleugels JLA, Kasi PM, Wallace MB. Colorectal cancer. Lancet. 2019; 394: 1467-1480.
- Van Cutsem E, Cervantes A, Adam R, Sobrero A, Van Krieken JH, et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann Oncol. 2016; 27: 1386-422.
- Engstrand J, Nilsson H, Strömberg C, Jonas E, Freedman J. Colorectal cancer liver metastases - a population-based study on incidence, management and survival. BMC Cancer. 2018; 18: 78.
- Abdalla EK, Vauthey JN, Ellis LM, Ellis V, Pollock R, et al. Recurrence and outcomes following hepatic resection, radiofrequency ablation, and combined resection/ablation for colorectal liver metastases. Ann Surg. 2004; 239: 818-25; discussion 825-7.
- Chakedis J, Schmidt CR. Surgical Treatment of Metastatic Colorectal Cancer. Surg Oncol Clin N Am. 2018; 27: 377-399.
- Shirakawa S, Kaneda K, Fujiwara H, Nishimura T, Sendo H, et al. [Case of a sigmoid colon cancer with metachronous metastases of the stomach and the abdominal wall]. Nihon Shokakibyo Gakkai Zasshi. 2009; 106: 653-9.
- Colloca GA, Venturino A, Guarneri D. Different variables predict the outcome of patients with synchronous versus metachronous metastases of colorectal cancer. Clin Transl Oncol. 2020; 22: 1399-1406.
- Cossu ML, Ginesu GC, Feo CF, Fancellu A, Pinna A, et al. Surgical outcomes in patients with hepatic synchronous and metachronous colorectal metastases. Ann Ital Chir. 2017; 88: 497-504.
- Tsai MS, Su YH, Ho MC, Liang JT, Chen TP, Lai HS, et al. Clinicopathological features and prognosis in resectable synchronous and metachronous colorectal liver metastasis. Ann Surg Oncol. 2007; 14: 786-94.
- Terashima S, Watanabe S, Kogure M, Tanaka M. Long-term survival after resection of a gastric metastasis from transverse colon cancer: a case report. Fukushima J Med Sci. 2019 Aug 30;65(2):37-42. doi: 10.5387/fms.2018-24.
- Kim DD, Park IJ, Kim HC, Yu CS, Kim JC. Ovarian metastases from colorectal cancer: a clinicopathological analysis of 103 patients. Colorectal Dis. 2009; 11: 32-8.
- Taylor AE, Nicolson VM, Cunningham D. Ovarian metastases from primary gastrointestinal malignancies: the Royal Marsden Hospital experience and implications for adjuvant treatment. Br J Cancer. 1995; 71: 92-6.
- Sugarbaker PH. Mechanisms of relapse for colorectal cancer: implications for intraperitoneal chemotherapy. J Surg Oncol Suppl. 1991; 2: 36-41.
- Sugarbaker PH. Laboratory and clinical basis for hyperthermia as a component of intracavitary chemotherapy. Int J Hyperthermia. 2007; 23: 431-42.
- Verwaal VJ, van Ruth S, de Bree E, van Sloothen GW, van Tinteren H, et al. Randomized trial of cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy and palliative surgery in patients with peritoneal carcinomatosis of colorectal cancer. J Clin Oncol. 2003; 21: 3737-43.
- Oda, Kondo H, Yamao T, Saito D, Ono H, Gotoda T, et al. Metastatic tumors to the stomach: analysis of 54 patients diagnosed at endoscopy and 347 autopsy cases. Endoscopy. 2001; 33: 507-10.
- Iwai N, Okuda T, Harada T, Oka K, Hara T, Inada Y, et al. Gastric Metastasis from Colorectal Cancer Mimicking a Submucosal Tumor. Case Rep Gastroenterol. 2020; 14: 338-345.
- Kwon J, Han HS, Kim HK, Baek SW, Yang Y, Lee KH, et al. Long-term Survival after Repeated Local Therapy and Salvage Chemotherapy for Recurrent Metastases from Gastric Cancer: a Case Report and Literature Review. J Gastric Cancer. 2018; 18: 305-312.