A rare case of severe PID caused by Raoultella ornithinolytica and Bacteroides fragilis
Mamukadze I*; Weiler E; Lindsey H
University of Michigan Health - Sparrow, 1200 East Lansing Michigan 48912, USA.
University of Michigan Health - Sparrow, 1200 East Lansing Michigan 48912, USA.
Background: Pelvic Inflammatory Disease (PID) is commonly caused by Sexually Transmitted Infections (STIs); however, non-STI pathogens contribute to only 15% of cases. Polymicrobial infections can lead to severe PID owing to bacterial synergy. The identification of bacteria is crucial for guiding antibiotic treatment. We report a case of PID infection with cultures indicating the presence of Bacteroides fragilis and Raoultella ornithinolytica, a bacterium not previously reported in the literature.
Case presentation: A 42-year-old female presented to the ER with acute lower abdominal pain. Laboratory tests showed leukopenia, thrombocytopenia, elevated lipase, and elevated total bilirubin levels. Imaging revealed scant fluid in the cul-de-sac. Diagnostic laparoscopy confirmed severe PID. Intraoperative cultures showed Raoultella ornithinolytica and Bacteroides fragilis. Antibiotics were changed to target the bacteria in the culture, and the patient quickly recovered and was discharged.
Discussion: Diagnosing PID is challenging because of inconsistent STI history and negative imaging findings. Notably, literature review revealed no prior cases of Raoultella Ornithinolytica causing PID, either alone or in combination with Bacteroides fragilis. The patient’s recent lake exposure may have contributed to the infection, as Raoultella ornithinolytica is found in the lakes. Synergistic effects between the pathogens likely precipitated the severe infections.
Conclusion: This case underscores the uniqueness of pathogen combinations in PID, highlighting the importance of considering rare pathogens in diagnosis. Clinicians should maintain a high clinical suspicion of PID, particularly in patients with atypical presentations or negative STI results.
Keywords: Pelvic inflammatory disease; Bacteroides fragilis; Raoultella ornithinolytica; Polymicrobial infection; Rare bacteria.
Manuscript Information: Received: Oct 23, 2024; Accepted: Nov 13, 2024; Published: Nov 20, 2024
Journal: Annals of Surgical Case Reports & Images
Online edition: https://annscri.org
Copyright: © Mamukadze I (2024). This Article is distributed under the terms of Creative Commons Attribution 4.0 International License.
Cite this article: Mamukadze I, Weiler E, Lindsey H. A rare case of severe PID caused by Raoultella ornithinolytica and Bacteroides fragilis. Ann Surg Case Rep Images. 2024; 1(6): 1058.
Pelvic Inflammatory Disease (PID) is a prevalent infection affecting female reproductive organs, including the uterus, fallopian tubes, and ovaries. Non-STI pathogens contribute to 15% of PID cases and are commonly associated with Sexually Transmitted Illnesses (STIs). Polymicrobial infections, characterized by bacterial synergy, can precipitate severe PID, surpassing individual virulence.
Non-STI-related PID pathogens include Staphylococcus, Klebsiella, Escherichia coli, Fusobacteria, Clostridia, and Actinomyces. Identifying these bacteria is crucial for effectively tailoring antibiotic therapy.
Here, we present a unique case of PID involving cultures positive for Bacteroides Fragilis and Raoultella Ornithinolytica, with the latter being an unprecedented cause of PID. This case underscores the necessity for comprehensive bacterial identification to optimize PID management, shedding light on the potentially overlooked pathogens in PID etiology.
A 42-year-old woman arrived at the Emergency Department (ED) with sudden lower abdominal pain that awoke her from sleep. The pain persisted at a constant intensity since its onset. She denied experiencing fever, chills, flank pain, hematuria, dysuria, vaginal bleeding, or discharge. Although she felt nauseous, she did not vomit or experience diarrhea. She also noted pain during intercourse over the past three days.
The patient had no history of Sexually Transmitted Diseases (STDs), had recent sexual activity with new partners, and had an exclusive relationship with her husband. She had recently visited Texas, where she swam in a lake, but had not traveled elsewhere.
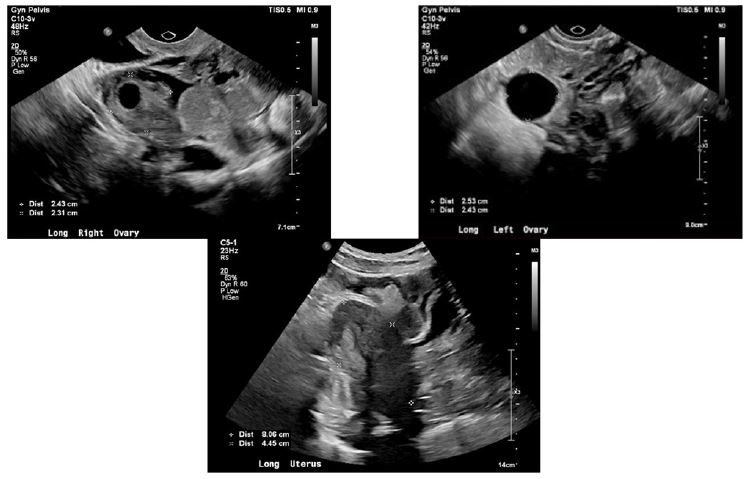
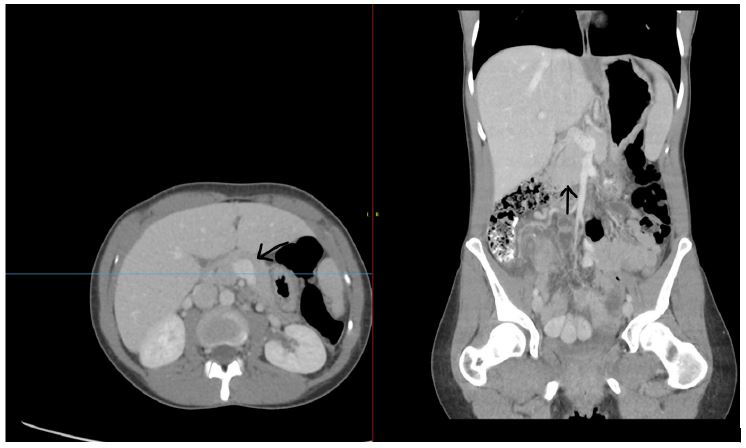
During examination, the patient displayed severe tenderness in the suprapubic and lower abdominal regions. Computed Tomography (CT) revealed a small amount of pelvic fluid in the posterior cul-de-sac, without significant findings. Pelvic ultrasonography has yielded inconclusive results (Figure 1). STD testing for Chlamydia, Gonorrhea, and Trichomonas returned negative results, as did urinalysis with culture. Laboratory tests showed leukopenia, platelet count of 108, lipase level of 1058, and a total bilirubin level of 1.6 with a mixed component.
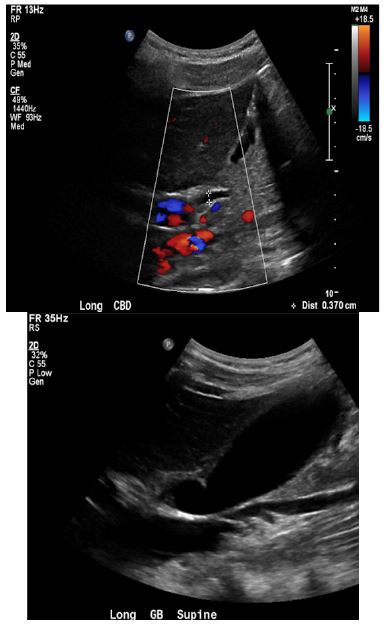
Further investigations via abdominal ultrasound and CT showed normal findings, including a normal-looking pancreas (Figures 2-4). The Gynecology (GYN) service concluded that abdominal pain likely stems from an issue unrelated to gynecology, possibly involving the abdominal or gastrointestinal (GI) tract. Consequently, the patient was admitted to the general surgery service with a suspected diagnosis of pancreatitis and was started on antibiotics (piperacillin and tazobactam/doxycycline).
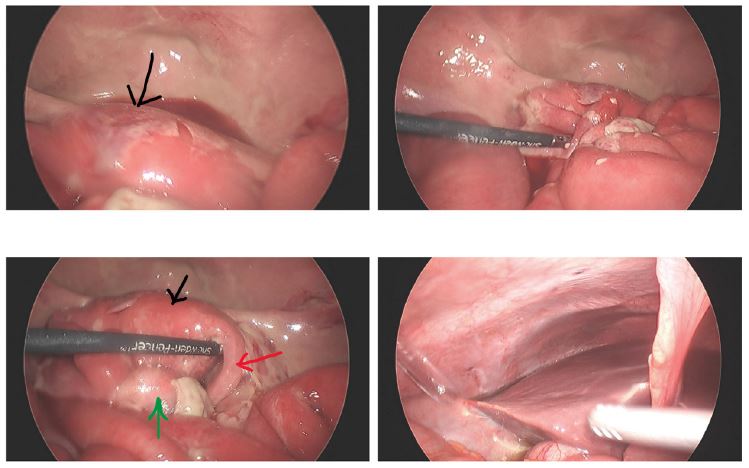
On the second day of hospitalization, the patient reported worsening abdominal pain in the suprapubic area accompanied by abdominal distension, diffuse tenderness, and peritoneal signs. Consequently, diagnostic laparoscopy revealed extensive inflammation involving the uterus, bilateral fallopian tubes, and left ovary. The right ovary was not visualized, and portions of the small bowel were adherent to the uterus and the left ovary. Abundant cloudy straw-colored fluid was observed in the abdominal cavity, and 100 mL was aspirated for further analysis.

A conclusive diagnosis of PID was made, prompting the adjustment of the antibiotic regimen to target the pathogens recognized for causing PID. The patient was then transferred to the Gynecology (GYN) Service for specialized care. Cultures from the abdominal fluid collection were positive for Raoultella ornithinolytica and Bacterioides fragilis. Antibiotic treatment was adjusted accordingly, and the patient was discharged on the third postoperative day without complications. A comprehensive plan for ongoing management and follow-up care was established to ensure the patient’s well-being.
The PID was diagnosed intraoperatively. The presence of elevated lipase levels, abnormal liver function test results, and non-specific findings on computed tomography further complicates the diagnostic process. Additionally, findings from the Study for Monitoring Antimicrobial Resistance Trends (SMART) program indicated that Klebsiella oxytoca (K.oxytoca) plays a significant role in Urinary Tract Infections (UTIs). The SMART program reported that K. oxytoca is responsible for approximately 0.7%-3.6% of UTI cases worldwide [3]. However, there are no documented case reports in the literature on this pathogen, either in isolation or in conjunction with Bacterioides fragilis, causing PID.
Klebsiella oxytoca and Raoultella ornithinolytica infections in humans are extremely rare. Historically, these pathogens have primarily been associated with aquatic environments. Their emergence as human pathogens was first documented in 2001 [2]. Interestingly, the patient mentioned swimming in a Texas lake five days before the onset of symptoms, which could explain the culture yielding Raoultella ornithinolytica. In contrast, Bacteroides fragilis is a component of the normal bacterial flora found in mucous membranes, including the gastrointestinal tract, oral cavity, and genital areas. Although B. fragilis is not typically an invasive enteric pathogen, it can cause infections such as PID if colonic contents contaminate the extra-intestinal host environment [1,4]. In this particular case report, it is conceivable that a synergistic effect between Bacteroides fragilis and Raoultella ornithinolytica contributed to the severe infection, resulting in an ascending infection causing pancreatic inflammation and elevated liver function.
The significance of this case report lies in its contribution to medical knowledge, role in facilitating early diagnosis and treatment, implications for public health, the potential to stimulate further research, enhancement of the differential diagnosis process, and educational value for healthcare professionals. This underscores the importance of recognizing and understanding less common pathogens within the context of common gynecological conditions such as PID.
This case highlights the challenges of diagnosing and treating PID when typical indicators are absent. The identification of rare pathogens emphasizes the need to consider environmental exposure. Surgical intervention was crucial for correct diagnosis and treatment. Maintaining a high suspicion of PID, especially in patients with suggestive symptoms and recent environmental exposures, is crucial for the timely management and prevention of complications.
Disclosure: The authors declare that they have no conflicts of interest or disclosures to report regarding the publication of this case report.
Declaration of generative AI and AI-assisted technologies in the writing process: During the preparation of this work, the authors used ChatGPT tool in order to improve the readability of the manuscript. After using this tool, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.
Data: The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Author contribution: Irada Mamukadze: Was involved in patient care, was involved in operating on the patient, and wrote manuscript.
Eric Weiler: Helped with writing the manuscript and collecting data.
Hugh Lindsey: Principle Investigator, was involved in patient care, was a primary attending surgeon in the case, and editing manuscript.
Patient consent statement
We hereby confirm that we have obtained written informed consent from the patient in this case report for the publication of their clinical information, including any accompanying images. The patient has been provided with a thorough explanation of the purpose of the case report, its potential publication, in scientific journals, and the possible dissemination of the information to the public.
The patient understands that their identity will remain confidential to the extent permitted by the law and that reasonable efforts will be made to conceal any personally identifiable information. However, it is acknowledged that complete anonymity cannot be guaranteed, particularly in the case of accompanying images or unique clinical circumstances.
The patient has been given the opportunity to ask questions regarding the case report, its publication, and the potential risks and benefits associated with disclosing their clinical information. They have provided their consent voluntarily, without coercion or undue influence, and understand that they have the right to withdraw their consent at any time prior to publication.
A copy of the signed informed consent form is available for review upon request.
Disclosures: Human subjects: Consent was obtained by all participants in this study.
Conflict of interest statement: The author declares that the case report was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
Data access statement: All relevant data are included in the manuscript.
Funding statement: This case report was not funded.