Introduction
Small Cell Lung Cancer (SCLC) is strongly associated with exposure to tobacco products and is marked by an exceptionally high proliferative rate, strong predilection for early metastasis, and poor prognosis [1]. Common routes of metastasis of SCLC include lymphatic spread to hilar and mediastinal lymph nodes and hematogenous spread to the contralateral lung, brain, liver, adrenal glands, and bone [2]. While SCLC metastasis to distant organs is well-documented, occurrences of metastasis to the nasopharynx are exceedingly uncommon and warrant further exploration.
Understanding the underlying mechanisms and clinical implications of rare metastatic disease is imperative to enhance diagnostic precision and tailor effective treatment strategies [3]. Early chemo radiation is the standard of care for limited-stage SCLC. Although most SCLCs initially respond to therapy, they have a propensity to recur [4]. This case furthermore exemplifies the critical role of early chemo radiation therapy in managing metastatic SCLC, emphasizing the importance of patient compliance in achieving optimal therapeutic outcomes [5-7].
In this case report, we aim to shed light on a rare SCLC metastasis and demonstrate the significance of patient engagement and support to achieve successful therapeutic interventions.
Case presentation
In this case report, we present a 63-year-old SCLC patient who was treated with chemo radiation to the lung at the time of initial diagnosis. However, he had a history of poor compliance with numerous missed treatments and was ultimately lost to follow-up. He subsequently presented two years later with rapidly worsening unexpected weight loss, dyspnea, dysphagia, dysphonia, right-sided V3 neuralgia, and right-sided nasal obstruction.
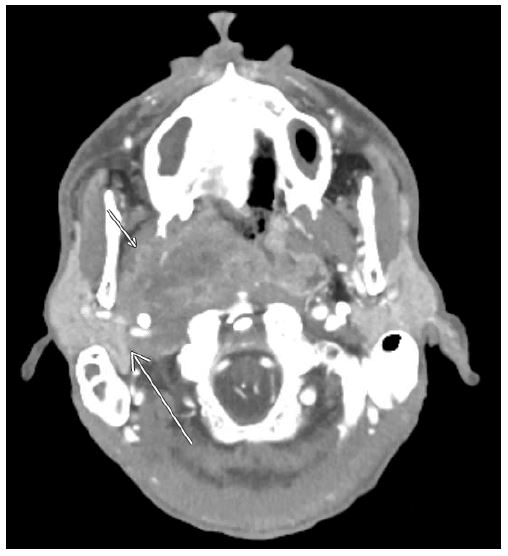
Flexible nasal endoscopy was significant for a hyperemic mass encompassing the entire posterior nasopharynx and sphenoethmoidal recess (Figure 1). Evaluation of the right true vocal cord showed paralysis and fixation in the paramedian position with a mobile left true vocal cord. Functional endoscopic evaluation of swallowing revealed significant residual pooling in the piriform sinuses and vallecula with penetration and aspiration of liquids. CT imaging revealed a locoregionally advanced nasopharyngeal mass with lateral extension to the deep lobe of the right parotid gland and complete effacement of the parapharyngeal space. Retropharyngeal lymphadenopathy was noted without any lateral cervical lymph nodes (Figure 2). The patient was admitted for nutritional optimization and a gastrostomy tube was placed during his inpatient stay.
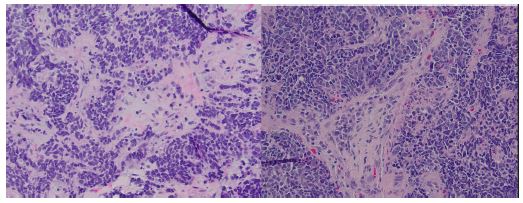
Biopsy of the right nasopharyngeal mass revealed malignant epithelial cells arranged in sheets. The tumor cells were cohesive with high nuclear-to-cytoplasmic ratios, hyperchromatic nuclei, and granular chromatin. The cells were positive for synaptophysin confirming neuroendocrine differentiation (Figure 3). After discussion at a multidisciplinary tumor conference and confirmation with the pathology team, consensus was reached that this was likely metastatic disease from incompletely treated SCLC.
Due to the extent of metastatic disease, multi-disciplinary recommendations were made for referral back to the oncology team for consideration of systemic therapy, the radiation oncology team for possible palliative radiation to the nasopharynx, and supplemental imaging studies to rule out intracranial involvement. Since the patient had concurrent moderate-to-severe conductive and sensorineural hearing loss, he was deemed to not be a good candidate for cisplatin/etoposide. Thus, carboplatin and etoposide chemotherapy was initiated along with radiation therapy. Magnetic resonance imaging two months after the CT scan revealed the nasopharyngeal mass, showed a progression of the solid mass arising from the right nasopharynx. The mass measured approximately 7.1 x 9.3 x 4.5 cm and was shown to obliterate the right parapharyngeal space, invade the adjacent right medial pterygoid muscle, encase the right internal carotid artery, obliterate the internal jugular vein, and invade the right side of the clivus. The mass was still shown to invade the deep and part of the superficial lobes of the right parotid gland (Figure 4). The mass also infiltrates the longus capitis muscles, right greater than left, and extends into the right nasal cavity and right pterygopalatine fossa. The previously noted right lateral retropharyngeal metastatic lymph node conglomerate was demonstrated on MRI to be congruent with the nasopharyngeal mass. No discrete intracranial extension is noted. No orbital or hypopharyngeal involvement is seen.
Since the initiation of chemoradiation therapy, the patient’s medical course has been complicated by hospital admission due to neutropenic infection (low WBC of 0.44). Multi-disciplinary medical treatment with oncology, radiation oncology, otolaryngology, and pulmonology continues as therapeutic management is maximized.
Discussion
Small Cell Lung Cancer (SCLC) is renowned for its aggressive nature, rapid proliferation, and propensity for early metastasis, often before clinical detection. Most patient have metastasis at the time of diagnosis, with less than 50% two-year survival and less that 5% five-year survival [8]. The high mitotic rate of SCLC lends to its aggressive behavior, contributing to the early formation of distant metastases [1]. The feature of propensity to metastasize sets SCLC apart from Non-Small Cell Lung Cancer (NSCLC) [9]. The most common sites of metastasis for SCLC include the liver, bones, adrenal glands, and brain [2]. The tumor’s extensive neuroendocrine features and high growth fraction contribute to the hematogenous and lymphatic spread [10].
Metastasis of SCLC to the nasopharynx represents a rare and intriguing clinical picture, diverging from the more typical sites of spread. The exact mechanism underlying this uncommon metastasis remains unclear, but one possible route could be hematogenous dissemination due to the rich vascularity and anatomical position of the nasopharyngeal region, allowing circulating tumor cells to infiltrate and establish metastatic lesions [11].
Management of SCLC requires comprehensive therapeutic strategies [3]. For patients with limited-stage SCLC, the standard of care involves early initiation of chemoradiation therapy. Combining chemotherapy, often platinum-based, with radiation aims to eradicate both local and systemic disease [7,12]. The success of this treatment modality is evident in the initial response of most SCLCs to therapy. However, despite a remarkable early response to treatment, recurrence is common [4].
The prominent trait of recurrence in SCLC draws attention to the need for consistent follow-up and vigilance in monitoring patients during and after treatment. Early detection of recurrence is crucial for ensuring swift therapy, potentially improving outcomes and quality of life for patients [5]. Adherence to recommended follow-up appointments, surveillance imaging, and, most importantly, chemo-radiation appointments is essential for optimizing outcomes [13]. Because SCLC requires a proactive treatment plan, a multi-disciplinary approach and efficient communication between providers and patients are vital for patient compliance and successful long-term management [6].
Conclusion
This case provides a prime example of the importance of consistent follow-up and compliance and some of the devastating, albeit rare, effects that can result from incompletely treated SCLC.
References
- Rudin CM, Brambilla E, Faivre-Finn C, Sage J. Small-cell lung cancer. Nat Rev Dis Primer. 2021; 7(1): 3. doi:10.1038/s41572-020-00235-0
- Nakazawa K, Kurishima K, Tamura T, et al. Specific organ metastases and survival in small cell lung cancer. Oncol Lett. 2012; 4(4): 617-620. doi:10.3892/ol.2012.792
- Ko J, Winslow MM, Sage J. Mechanisms of small cell lung cancer metastasis. EMBO Mol Med. 2021; 13(1): e13122. doi:10.15252/emmm.202013122
- Van Meerbeeck JP, Fennell DA, De Ruysscher DKM. Small-cell lung cancer. Lancet Lond Engl. 2011; 378(9804): 1741-1755. doi:10.1016/S0140-6736(11)60165-7
- Megyesfalvi Z, Gay CM, Popper H, et al. Clinical insights into small cell lung cancer: Tumor heterogeneity, diagnosis, therapy, and future directions. CA Cancer J Clin. 2023; 73(6): 620-652. doi:10.3322/caac.21785
- Hartigan K. Patient education: The cornerstone of successful oral chemotherapy treatment. Clin J Oncol Nurs. 2003; 7(6 Suppl): 21-24. doi:10.1188/03.CJON.S6.21-24
- Baldini E, Kalemkerian G. Limited-stage small cell lung cancer: Initial management. UpToDate. 2023. https://www.uptodate.com/contents/limited-stage-small-cell-lung-cancer-initial-management
- Basumallik N, Agarwal M. Small Cell Lung Cancer. In: StatPearls. StatPearls Publishing. 2023. http://www.ncbi.nlm.nih.gov/books/NBK482458/
- Clark SB, Alsubait S. Non-Small Cell Lung Cancer. In: StatPearls. StatPearls Publishing. 2023. http://www.ncbi.nlm.nih.gov/books/NBK562307/
- Xie S, Wu Z, Qi Y, Wu B, Zhu X. The metastasizing mechanisms of lung cancer: Recent advances and therapeutic challenges. Biomed Pharmacother Biomedecine Pharmacother. 2021; 138: 111450. doi:10.1016/j.biopha.2021.111450
- Liu JC, Kaplon A, Blackman E, Miyamoto C, Savior D, et al. The impact of the multidisciplinary tumor board on head and neck cancer outcomes. The Laryngoscope. 2020; 130(4): 946-950. doi:10.1002/lary.28066
- Rossi A, Di Maio M, Chiodini P, et al. Carboplatin- or cisplatin-based chemotherapy in first-line treatment of small-cell lung cancer: the COCIS meta-analysis of individual patient data. J Clin Oncol Off J Am Soc Clin Oncol. 2012; 30(14): 1692-1698. doi:10.1200/JCO.2011.40.4905
- Tariq S, Kim SY, Monteiro de Oliveira Novaes J, Cheng H. Update 2021: Management of Small Cell Lung Cancer. Lung. 2021; 199(6): 579-587. doi:10.1007/s00408-021-00486-y