Introduction
Lower limb wounds with exposed implants, tendons or extensive degloving with large soft tissue defects pose a significant challenge for the reconstructive surgeon. The traditional reconstruction ladder concept advocates choosing the simplest reconstruction technique needed for the defect, advancing further along the ladder only if necessary [1]. With the shift towards the reconstruction elevator where the best option for reconstruction is undertaken regardless of complexity, there has been a tendency towards performing free flap surgeries. However free flap surgeries are expensive, longer in duration, result in donor site morbidity and have non-negligible failure rates [2]. In lower limb wounds where dynamics and contour are very important to restore normal function, free flaps may not be the best solution as they are often bulky.
Dermal matrixes such as MatriDerm® (Dr. Otto Suwelack Skin & Health Care AG, Billerbeck, Germany), NovoSorb™ (Polynovo, Adelaide, Australia) and Kerecis® (Kerecis, Isafjordur, Iceland) serve as a scaffold for dermal regeneration in wounds and should not be viewed as an inferior alternative for patients who are poor surgical candidates. MatriDerm® is a single-layer bovine collagen-elastin template that can be applied both in a one- and multi-step procedure. NovoSorb™ is a bilayer fully synthetic dermal substitute composed of a biodegradable polyurethane foam. Kerecis® is composed of intact fish skin from Icelandic Cod and is structurally similar to human skin, supporting cell and vascular ingrowth. All these dermal substitutes have the advantages of being unlimited in quantity, can be trimmed to conform to any defect and have lower operative risk. Traditionally used to cover extensive burns, their application has since been extended to resurface traumatic wounds and chronic ulcers where they have been shown to increase the elasticity and pliability of the reconstructed skin [3,4].
In our paper, we present our experience in the reconstruction of 6 challenging lower limb wounds utilizing dermal matrices paired with negative pressure wound therapy and subsequent split skin grafting.
Case series
Case 1
A 72-year-old lady with a history of bilateral lower limb chronic venous insufficiency developed necrotising fasciitis in her left calf secondary to an infected venous ulcer. She underwent emergency surgical drainage and was noted to have posterior lateral compartment necrotising fasciitis with necrotic fat and copious pus from liquefactive necrosis. The muscle tissue had borderline viability and skin flaps were dusky. Loculations were released and the wound bed was washed with 6L of normal saline using the Pulsavac® system. Necrotic tissue was debrided extensively and V.A.C.® Therapy applied. The patient underwent 3 further debridement operations until a clean wound bed was achieved. Subsequently, Kerecis® sheets were trimmed to size and applied to cover the whole wound. V.A.C.® Therapy was placed over Kerecis® and changed every 3 days with the fish-skin matrix left in situ. After 6 V.A.C.® Therapy changes, healthy granulation tissue was noted over the wound bed and split skin grafting was performed with ipsilateral thigh skin. The skin graft took well and on follow up in the outpatient clinic 3 months post skin grafting, all wounds had fully epithelised and patient was ambulating well.
Case 2
The second patient was a 68-year-old gentleman with peripheral vascular disease and diabetes mellitus. He presented with an infected transmetatarsal amputation wound that had broken down. After repeat debridement and drainage to eradicate the infection, he was left with a sizeable wound with degloving and dead space. He was a poor candidate for free flap surgery due to poor vascularity despite revascularization attempts. Although more commonly performed in a single stage fashion, decision was made to use 2 mm thick MatriDerm® sheet in a delayed manner to allow more granulation tissue to form prior to skin grafting as there was a thin interface between the wound surface and underlying bone. The wound was subjected to conventional V.A.C.® Therapy with regular biweekly change. At the 22nd day mark, the wound bed was healthy and split skin grafting was performed. At clinic review 5 months post operatively, the wounds were all healed and the patient was able to ambulate without aids using a modified shoe.
Case 3
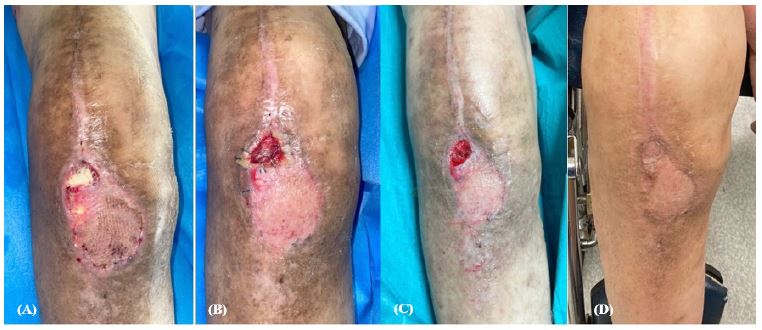
A 61-year-old gentleman presented with a chronically infected right total knee replacement wound. After repeated debridement and washouts, the implant was replaced and the wound covered with a gastrocnemius flap combined with split skin grafting. However, at 2 weeks post operatively there was dehiscence of the flap tip with resultant exposure of the underlying implant. The bilayer NovoSorb™ temporizing matrix was applied to the wound with skin staplers and V.A.C.® Therapy applied over. V.A.C.® Therapy was changed every 3 days and on the 4th dressing change, the matrix was determined to have integrated as there was capillary refill and healthy colouration. The superficial sealing membrane was then removed and healthy granulation tissue was observed. Split skin grafting was performed and at outpatient review 3 months post operatively, the patient was ambulating well with satisfactory knee range of motion of 0 to 110 degrees.
Case 4
The fourth patient was a 64-year-old gentleman with a background of poorly controlled diabetes. He was referred for worsening left heel ulcer with exposed tendo-achilles. The wound had developed as result of him wearing ill-fitting boots at his job as a construction supervisor. On initial presentation, the wound was sloughy and malodorous. The patient underwent 3 rounds of surgical debridement and V.A.C. VERAFLO™ therapy to remove biofilm and decrease the bacterial load in the wound. Kerecis® was applied to the wound with staplers and conventional V.A.C.® Therapy over. After 2 weeks of V.A.C.® Therapy changes, healthy granulation tissue was observed at the wound bed and split skin grafting performed. The patient recovered well and had returned back to work at the 6th month clinic review.
Case 5
The fifth patient was a 51-year-old lady with a history of poorly controlled diabetes mellitus. She developed a third toe ulcer with exposed extensor tendon after debridement. NovoSorb™ was applied to the wound and V.A.C.® Therapy placed over. V.A.C.® Therapy was changed every 3 days and after the 2nd dressing change, the sealing membrane was removed revealing healthy granulation tissue under. Split skin grafting was performed and at outpatient review 2 months post operatively, the patient was ambulating well and able to wear normal footwear.
Case 6
An elderly 75-year-old gentleman with multiple comorbidities and Alzheimer’s disease was referred with an infected left foot wound with exposed extensor tendons without paratenon. As the patient was a poor surgical candidate for free flap surgery, he underwent repeat wound debridement and V.A.C. VERAFLO™ therapy before MatriDerm® application. A 2 mm thick MatriDerm® sheet was applied in a delayed fashion again to allow more granulation tissue to form over the extensor tendons. The wound was subjected to conventional V.A.C.® Therapy with regular biweekly change. At the 21 day mark, there was tissue and vascularization ingrowth into the matrix and split skin grafting was performed. At clinic review 5 months post operatively, the wounds were all healed with good contour and function. Patient was able to wear normal footwear without any issues.
Discussion
Wounds, particularly chronic wounds, are a major health issue in first and third world countries alike. Globally, the prevalence of chronic wounds is estimated at 1.51 to 2.21 per 1000 population [5]. This incidence is expected to rise with ageing populations worldwide. A United States census found that approximately 8.2 million of the population had wounds, with cost estimates for acute and chronic wound treatments ranging from $28.1 billion to $96.8 billion [6]. In Singapore, a 2017 population-based study found that the incidence of any wound was 300 per 100 000 persons in the general population and 800 per 100 000 among those aged 50 and older [7]. Chronic wounds reduce the quality of life of patients, affect their physical and mental wellness, and pose a significant financial burden both on an individual and societal level [8]. This has led to greater interest in the utility of wound products such as dermal matrices in the management of complex wounds.
Dermal matrices are increasingly becoming an essential tool in the reconstructive surgeon’s toolbox. First introduced clinically in 1994 for the management of full-thickness burns, they have since become an integral part of the management of abdominal wall defects, chronic wounds and capsular contracture [9]. Dermal matrices function as a soft connective tissue graft upon which the patient’s native cells can colonize and vascularize, serving as a scaffold to provide greater structural integrity [10]. They may be acellular or retain biological components most commonly from bovine, porcine or piscine origin.
In the field of wound management, traditional teaching advocates the use of flap based reconstruction when wounds have exposed vital structures such as tendons, bones and implants. However, our case series shows that when combined with V.A.C.® Therapy, dermal matrices can be built up to provide sufficient coverage almost equivalent to a flap. Previous authors have also reported successful resurfacing of exposed joints and tendons with dermal matrices and skin grafting in a single stage approach [11,12]. Similar to Shah et al. [13], we prefer to use a 2 stage approach based on the concept of sequential revascularization, delaying the split skin grafting until the dermal matrix has been adequately integrated. This allows wounds with suboptimal vascularity to be covered gradually over time as the dermal matrices are incorporated, allowing for sufficient neovascularization of the wound bed prior to split skin grafting. In all 6 of our cases, no graft loss was observed. In contrast, success of the single stage approach would be dependent on the wound’s ability to revascularize both the dermal matrix and the split skin graft rapidly before the skin graft begins to desiccate and necrose.
Cases 1 and 2 illustrate the advantage of dermal matrixes in large wounds where skin grafting alone would lead to greater contour irregularity and a less pliable, more contracted scar with threatened exposure of underlying structures. Conversely, flap based reconstruction would be difficult due to the need for large and thin dimensions. Furthermore, in case 1, a single flap may not suffice. In such situations, dermal matrixes -with their unlimited nature and improved skin quality and elasticity- are excellent solutions. In a retrospective review of 78 patients who had undergone skin grafting with or without dermal matrix, Park et al. found that in the group of patients who received the dermal matrix, skin quality was more superior by both subjective and objective assessments [14].
Cases 3,4 and 5 demonstrate the usefulness of dermal matrixes in small wounds with crucial defects where skin grafting alone cannot provide sufficient coverage but flap reconstruction would be excessive.
Case 6 exemplifies the utility of dermal matrixes in patients with poor premorbid function where long flap surgeries would be deemed too high risk. Additionally, flap reconstruction in this region often necessitates subsequent debulking procedures for better contour and to enable the patient to wear normal footwear comfortably. Due to exposed paratenon in this case, the wound required a longer time to granulate before skin grafting but the eventual skin graft still took well.
V.A.C.® Therapy played a key role in our case series. We utilized the negative pressure wound care system in all of our cases at 125 mmgHg medium intensity with dressing change performed every 3 days, leaving the underlying dermal matrix in place. V.A.C.® Therapy and dermal matrixes work synergistically. Besides maintaining maximal adhesion of the dermal matrix to the wound bed and reducing bacterial load in a closed system, V.A.C.® Therapy also functions to stimulate granulation tissue and contract the wound, inducing angiogenesis thereby increasing blood flow to the wound bed. It draws the cellular factors for rebuilding to induce ingrowth into the scaffold provided by the dermal matrix [15].
Conclusion
In conclusion, dermal matrices should be recognized as an essential tool in the reconstructive surgeon’s armamentarium. Their application is particularly useful for patients who are poor surgical candidates for free flap surgery, in wounds with substantial soft tissue loss, as well as in minute but crucial wounds with exposed implants or tendons.
References
- Farid M, Friebel T, Nikkhah D. Decision-Making in Flap Surgery: Reconstructive Ladder versus Elevator. In: Nikkhah D, Rawlins J, Pafitanis G. (eds) Core Techniques in Flap Reconstructive Microsurgery. Springer, Cham. 2023: 19-24.
- Koster ITS, Borgdorff MP, Jamaludin FS, et al. Strategies Following Free Flap Failure in Lower Extremity Trauma: A Systematic Review. JPRAS open. 2023; 36: 94-104.
- Choi JY, Kim SH, Oh GJ, et al. Management of defects on lower extremities with the use of matriderm and skin graft. Arch Plast Surg. 2014; 41(4): 337-343.
- Min JH, Yun IS, Lew DH, et al. The use of matriderm and autologous skin graft in the treatment of full thickness skin defects. Arch Plast Surg. 2014; 41(4): 330-336.
- Martinengo L, Olsson M, Bajpai R, et al. Prevalence of chronic wounds in the general population: Systematic review and meta-analysis of observational studies. Annals of epidemiology. 2019; 29: 8-15.
- Sen CK. Human Wounds and Its Burden: An Updated Compendium of Estimates. Advances in wound care. 2019; 8(2): 39-48.
- Goh OQ, Ganesan G, Graves N, et al. Incidence of chronic wounds in Singapore, a multiethnic Asian country, between 2000 and 2017: A retrospective cohort study using a nationwide claims database. BMJ Open. 2020; 10: e039411.
- Zhu X, Olsson MM, Bajpai R, et al. Health-related quality of life and chronic wound characteristics among patients with chronic wounds treated in primary care: A cross-sectional study in Singapore. Int Wound J. 2022; 19(5): 1121-1132.
- Daar DA, Gandy JR, Clark EG, et al. Plastic Surgery and Acellular Dermal Matrix: Highlighting Trends from 1999 to 2013. World journal of plastic surgery. 2016; 5(2): 97-108.
- Wong AK, Schonmeyer B, Singh P, et al. Histologic analysis of angiogenesis and lymphangiogenesis in acellular human dermis. Plast Reconstr Surg. 2008; 121: 1144-52.
- Kakagia DD, Georgiadis G, Drosos G. Dermal Matrices: Game Changers in Leg and Foot Soft Tissue Reconstruction? A Case Series. The international journal of lower extremity wounds. 2023; 22(1): 56-62.
- Li G, Shen Q, Zhou P, et al. Acellular dermal matrix for one-stage treatment of lower extremity full-thickness skin defect: a case series. BMC Surg. 2023; 23: 17.
- Shah A, Taupin P. Strategies for extremity reconstruction with exposed bones and tendons using acellular dermal matrices: concept of sequential vascularization. Case reports in plastic surgery & hand surgery. 2021; 9(1): 7-14.
- Park JY, Lee TG, Kim JY, et al. Acellular Dermal Matrix to Treat Full Thickness Skin Defects: Follow-Up Subjective and Objective Skin Quality Assessments. Archives of craniofacial surgery. 2014; 15(1): 14-21.
- Menn ZK, Lee E, Klebuc MJ. Acellular dermal matrix and negative pressure wound therapy: A tissue-engineered alternative to free tissue transfer in the compromised host. Journal of reconstructive microsurgery. 2012; 28(2): 139-144.