Introduction
Intra-articular injuries of the hip are being diagnosed with increasing frequency as diagnostic testing and surgical techniques to manage these injuries have improved [1-5]. Specifically, athletes are at considerably increased risk of hip and groin injuries, with pain in this region being reported by up to 23% of competitors each year [6-11]. Injuries about the hip joint can be complex and difficult to diagnose due to the vague nature of the clinical presentation [1]. Extra-articular injuries of the hip are the most common and are diagnosed at varying rates depending on the sport that the patient is playing. Studies have shown adductor and/or hamstring injury frequencies of up to 16% in soccer players, hip flexor strains in up to 3.1% in American Football players, and hamstring strains in 6.2% of basketball players [7-23]. In contrast, intra articular injuries of the hip are much less common in athletes and are sparsely reported in the literature.
Intra-articular pathologies of the hip are often more difficult to diagnose and can present with vague or nonspecific symptoms. Patients will often present with anterior or posterior hip pain. Less often the pain will be localized laterally. The pain may be described as a dull ache, or sharp in nature. Oftentimes symptoms of lumbar radiculopathy can overlap with symptoms of intra-articular hip pathology, however, this is less of a problem in the young athletic patient cohort and can be differentiated if the patient is having back pain or radicular symptoms. A thorough history and physical exam should be performed on patients presenting with hip pain to properly eliminate lumbar spinal pathology from the differential diagnosis.
Once lumbar pathology is ruled out, focus on appropriate diagnosis of hip pathology can begin. There is a wide array of intra-articular pathologies that exist, all of which should be considered. When considering hip pain in young athletes, the presence of a cam or a pincer lesion should always be considered. A cam lesion is defined as an aspherical femoral head that can lead to impingement of the hip joint and can even lead to labral tears, most often anterosuperiorly. A pincer lesion is defined as excessive overhang of the acetabular cup that can lead to hip impingement specifically with flexion and internal rotation as well as labral tears. Both presents with nonspecific symptoms similar to other intra-articular pathologies. In addition to the pain and impingement from these primary lesions, they can lead to concomitant pathologies within the hip joint. Because these lesions can be present in young athletes, they should always be considered when evaluating athletes with hip pain. Both cam and pincer lesions can be evaluated on x-ray with MRI used to further evaluate intra-articular sequelae that can arise.
Additional differential considerations for young athletes with suspected intra-articular hip pain includes labral tears, loose bodies, Femoroacetabular Impingement (FAI), capsular laxity, Ligamentum Teres (LT) rupture, and chondral damage [22]. Often these pathologies occur in association with one another. Labral tears can be a painful and debilitating injury in all patients, but athletes specifically, with these individuals at potentially increased risk of symptomatic tear. Most often a labral tear is located at the anterosuperior aspect of the joint and associated with pivoting or twisting of the lower extremity [15]. The anterior labrum is wider and thinner than the posterior, which may contribute to the higher frequency of tears in this location [9]. In the United States posterior labral tears are rare but may occur in the setting of trauma such as car accidents or falls [18]. In these instances, the force is directed through the femur, thus driving the femoral head posterior, causing damage to the posterior labrum [16]. While labral tears are most frequently encountered in the anterosuperior aspect of the acetabulum, our group has observed a disproportionate number of posterior labral tears in American Football players. The purpose of this study is to identify the type and location of intra-articular hip pathology in American Football players and to describe return to play following these injuries.
Materials and methods
Formal institutional board review approval was obtained (University of Missouri, IRB #2004777); patient consent was waived. A retrospective search of all radiology reports from 2007-2019 was performed to identify all Magnetic Resonance (MR) examinations of the hip requested by a single orthopedic team physician of a Midwest Division I college football program. Only individuals who were team members with a dedicated MR examination of the hip were included in the study. Patient names were cross checked with official roster designations which were publicly available via the team website. Inclusion criteria were any collegiate football player undergoing MR for a presumed diagnosis of acute intra-articular hip pathology. Exclusion criteria included non-football players, as well as patients being examined for extra-articular injury (hamstring strain, quadriceps injury), as well as those undergoing MR for evaluation for femoral neck stress fracture. Additionally, any patient who was undergoing a postoperative imaging exam, or an exam as part of routine screening was excluded. Return to play was determined by reference with the team website.
Imaging parameters
Our institution interprets MR imaging examinations from a variety of centers, which have different scanners and imaging techniques. All the MR examinations were performed on either a 3-T clinical scanner (Signa Excite, GE Healthcare) or a 1.5-T clinical scanner (Espree, Siemens Healthcare; Genesis Signa or Signa HDxt, GE Healthcare. Each examination used a dedicated hip coil with the patient’s hip placed in a neutral position.
Coronal T1-weighted image of the entire pelvis was obtained. Fat-suppressed Fast Spin-Echo (FSE) intermediate- or T2- weighted images were obtained in the axial, coronal, or sagittal planes in all patients. Proton density images were also obtained in the sagittal plane. The TR range and TE range were 1110 to 6300 and 11 to 52, respectively, and the echo train length was between 1 and 13. The slice thickness ranged between 3 and 4 mm, with an interslice gap of 1 mm. The number of excitations was either 1 or 2, and a flip angle of 90 degrees was used. A 16-cm field of view was used for all sequences with matrix size ranges of 256 to 640 and 216 to 640.
In six individuals, MR arthrography was performed. Following sterile skin preparation and local anesthesia of 1% lidocaine, fluoroscopic guidance was utilized to advance a 22-gauge spinal needle into the hip joint. A total of 12 cc. of the following mixture was injected (10 cc. normal saline, 5 cc. 0.25% Bupivacaine, 5 cc. Omipaque 300 and 0. 1 cc. Multihance (gadobenate dimeglumine)). Coronal, sagittal and oblique axial TI weighted fat suppressed images were obtained.
Magnetic resonance imaging interpretation
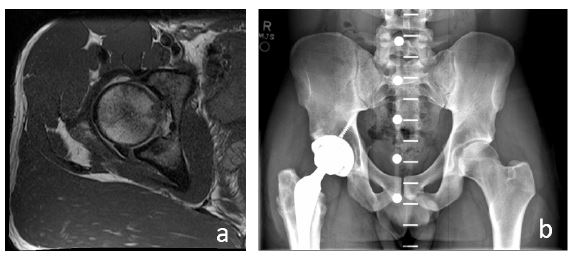
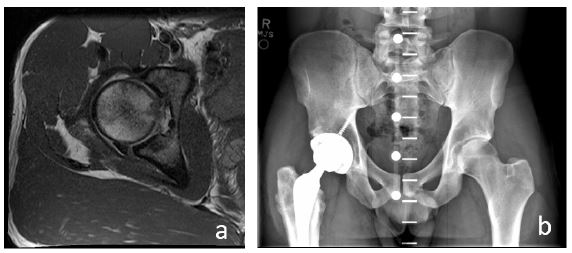
Two fellowship-trained musculoskeletal radiologists reviewed the MR hip exams by consensus. The following criteria were recorded: presence and location of a labral tear (Figure 1), fracture (Figure 2), and cartilage lesions. For cartilage and labral abnormalities, location was defined by dividing the hip into three equal segments, anterior, superior, and posterior. If an abnormality involved more than one segment, each segment involved was recorded individually. Finally, the LT was determined to be intact or torn.
A labral tear was defined by a linear signal abnormality through the entire thickness of the fibrocartilage. The presence of a fracture was determined as an area with linear low signal abnormality in the bone with or without marrow edema. The presence of articular cartilage defects was determined as high signal defects in the hyaline cartilage of either the femoral head or acetabulum with partial and complete defects combined as examples of abnormal. Partial and complete tears of the LT were defined as partial or full-thickness fiber disruption respectively.
Results
A total of 14 male football players were included in the study. The mean age was 21 years, and the ages ranged from 18-23 years old. A summary of the distribution of intra-articular injury can be found in Table 1. Sixteen labral tears were identified in 10 individuals with nearly equal distribution regarding location. Tears were in the anterior labrum in 70% of cases (7/10) compared to both the superior and posterior labral tears noted in 50% of cases (5/10). MRI imaging from a patient with a posterior labral tear demonstrated in Figure 1. Seventeen cartilage abnormalities were found in 9 out of the 14 individuals (64.3%), most commonly presenting in the superior portion of the joint noted in 66.7% of cases (6/9). Four of the 14 had acetabular fractures (28.6%). All 4 of these (100%) fractures involved the posterior wall. Three of the 14(21.4%) patients had an LT tear. All t3 tears (100%) were partial in nature.
64.2% (9/14) of individuals were able to return to play. Among the 5 individuals that were unable to return to play, the most common intra-articular finding was cartilaginous disruption which was present in all 5(100%). Second to this was a finding of a labral tear, which was present in 4 of the 5 individuals (80%). One of the 5 individuals (20%) who was unable to return to play suffered a posterior wall acetabular fracture. In this case, there were associated chondral injuries evident on MRI with subsequent avascular necrosis and collapse of his femoral head. This led to an eventual transition to a total hip arthroplasty (Figure 2).
When cartilage lesions were identified, these were most often acetabular rather than femoral. Nine out of 14(64.3%) of patients were noted to have chondral injury, with several patients having more than one defect noted (Table 1). There is no evidence that any of these cartilage lesions were related to a dislocation event. Two of the 14(14.2%) players had no evidence of any intra-articular injury.
Table 1: Summary of intra-articular injuries in american football players.
|
Labral Tears (N=10) |
| Anterior |
7 |
| Superior |
5 |
| Posterior |
5 |
|
Cartilage Lesions (N=9) |
| Anterior Acetabulum |
2 |
| Superior Acetabulum |
6 |
| Posterior Acetabulum |
4 |
| Anterior Femoral Head |
2 |
| Superior Femoral head |
3 |
| Posterior Femoral Head |
0 |
|
Fractures (N=4) |
| Posterior Acetabulum |
4 |
|
Ligamentum Tears Tear (N=3) |
| Partial |
3 |
Discussion
Our study identified intra-articular injuries in 12 of 14(85.7%) collegiate level American Football players who underwent MRI for presumed hip injury. Ten out of 14(71.4%) of these players had labral tears present on MR with 5/10 (50%) of those tears being posterior. The least common location for cartilage abnormalities was the anterior portion of the joint with superior and posterior chondral lesions more common. To our knowledge, no prior study has investigated the location of labral and chondral injuries in American Football players. Our results suggest posterior joint pathology occurs at higher rates in this population compared to the general population, where labral tears are most often anterosuperior [18]. Less common injuries in our study included disruption of the LT and fractures of the posterior acetabular wall. Although a history of the mechanism of injuries was not possible, we suspect the injury is most likely secondary to posterior translation of the femoral head following a fall on the flexed knee. This has previously been described as a potential mechanism of injury in American Football players and would explain the high incidence of posterior joint pathology [16].
Few studies have investigated intraarticular hip pathology in American Football. A study by Makovicka et al. examined 1,618 hip injuries over a ten-year period in the National Collegiate Athletic Association (NCAA) [14]. In this study, muscle strains accounted for over 75% of the hip injuries, with only 13 cases (0.8%) of hip subluxation or dislocation [14]. Only 1 case (0.06%) of a labral tear was documented, although the authors did not disclose the location of the tear [6]. Despite the apparent rarity of intra-articular injuries of the hip, these injuries often lead to increased time lost and possible long-term complications. A study of hip injuries in NFL players by Feeley et al. found the average time lost during an intra-articular injury to be 94.5 days with many of the patients experiencing persistent groin pain following the injury [8].
On the contrary, labral tears may be more common than the prior study indicates. A study by Domb et al. showed a labral tear rate of 89% in retired National Football League players with continued hip or groin pain [6]. This study examined 62 symptomatic hips in patients with a mean age of 33 years old [6]. The mean time since retirement was 2.9 years [6]. They found labral tears in 55(89%) of these hips, chondral lesions in 61(98%) and LI tears in 50(81%) of individuals [6]. The high rate of pathology in the study by Domb et al. can most likely be explained by the long-term, high impact nature of professional football in individuals older than our study group.
Treatment options for labral tears of the hip are typically tailored specifically to the patient and their needs. While labral tears on older patients with early onset arthritis may be treated nonoperatively with expectant management, those that occur acutely in young patients may be candidates for arthroscopic debridement or even repair or reconstruction. Hip preservation techniques, specifically hip arthroscopy, is a growing field of literature in orthopedics with data showing mixed, and often surgeon dependent results. Data on which patients in our cohort were treated operatively or non-operatively for a labral tear was not available, however, literature supports return to play after either operative or nonoperative treatment for football players with simple labral tears regardless of the location of the tear [8].
Cartilage injuries have been reported at varying rates among American football players. As mentioned above, Domb et al. found chondral lesions on MR in 61 out of 62 hips among retired NFL players with continued hip pain [6]. Feeley et al. studied all reported hip injuries in NFL players from 1997 to 2006 [8]. Of the 738 injuries, only 5% were noted to be intra-articular; however, cartilage injuries were not specified in this population [8]. To our knowledge, no additional studies have specified the role of cartilage lesions in football players. Our study adds to the literature, both by identifying that cartilage lesion will often accompany other intra-articular hip pathology, and by identifying that it is most prevalent both superior, and posterior within the acetabulum. Current treatment options for cartilage lesions of the hip are limited compared to other joints such as the knee, and this can be a serious injury, especially in younger athletes.
Tears of the LT was noted in 3/14 (21.4%) of our patients. Recently, there has been increased discussion in the literature regarding LT injuries and the role of repair and debridement. Multiple reports have linked LI rupture to hip micro instability, which can present as acute or chronic hip pain [4,12,24]. The proposed mechanism of LT’ rupture is a posteriorly directed force on a flexed and adducted knee, or sudden external rotation of the hip [3,19]. As such, IT injury has been noted American Football players as well as hockey players and skiers [3]. Despite LT injury commonly presenting during traumatic hip injuries, it is uncommon for surgeons to perform IT reconstruction during hip arthroscopy. A study by Bodendorfer et al. compared outcomes in patients with labral tears and concomitant LT tears to patients with isolated labral tears [2]. After labral repair in both groups, no significant difference in outcomes were noted [2]. LT reconstruction may still be indicated for patients with persistent pain or instability after primary hip arthroscopy, as patients have shown symptomatic improvement with revision arthroscopy and LT repair [13,21].
Traumatic posterior instability of the hip can be a serious cause of intra-articular injury that may be misdiagnosed as a simple strain [18]. Most of the literature consists of case reports and small studies with various outcomes, and sequelae. Case reports have described football related injuries leading to posterior dislocation of the hip with femoral epiphysis separation in a 13-year-old boy, as well as posterior dislocation in 22-year-old NCAA football player requiring chondral debridement and labral repair [17,20]. Moorman et al. studied traumatic posterior hip subluxation in 8 American Football players [24]. The injury mechanism was similar in all patients, with a fall on a flexed and adducted hip [24]. The authors discovered a similar imaging triad with all patients showing a posterior acetabular fracture, disruption of the iliofemoral ligament, and hemarthrosis [24]. Six players were able to return to their previous level of play, while two players developed osteonecrosis and eventually were treated with total hip arthroplasty [24]. We suspect a similar mechanism of injury likely caused the injuries in our cohort.
Management of posterior joint instability begins with activity modification combined with physical therapy, but surgical intervention may be necessary in more severe cases, or those refractory to non-operative management [18]. Complications following the injury include osteoarthritis, vascular necrosis, heterotopic ossification, thromboembolism, and sciatic nerve injury [14]. Because of the potential long-term severity, it is important that these injuries are identified and managed appropriately. A high level of suspicion should be present amongst football athletes due to the high energy mechanisms they are exposed to during competition. This was notable within our small cohort, in which one patient out of 4 who suffered acetabular fractures (25%) eventually required hip arthroplasty secondary to Avascular Necrosis (AVN).
Osteonecrosis of the hip is a devastating complication for a young athlete with limited treatment options. Non-operative treatment typically has a limited role due to the high levels of progression which can lead to collapse of the femoral head. If hip AVN is recognized early, one of the early treatment options is a core decompression which involves drilling into the center of the femoral head with hopes of halting the progression. A systemic review and meta-analysis by Hua et al. found mixed results in the literature, however, reported an overall success rate, defined as no need for conversion to THA at 65% [10]. The authors of this study did recommend the importance of only utilizing core decompression for early AVN as use later in the course can exacerbate hip osteonecrosis [10]. Once progression has gone beyond the initial stage, the arthroplasty is often the treatment of choice. Additional treatment options such as cephalomedullary nails or dynamic hip screws have been discussed with varying results and with select use cases based on patient history and examination.
This study is not without limitations. First this is a single institution, retrospective study, and as such suffers from limited history and small sample size. Despite this, we believe this to be the largest cohort of American Football players in which the location of labral and chondral pathology was investigated. Details regarding mechanism of injury, duration of symptom and treatment were not available as definitive treatment of all individuals occurred via physicians outside of our institution. Ultimately our goal was to describe the intraarticular imaging findings consistent with this injury, so that it may be better presented in the literature.
Conclusion
Our MR evaluation of American football players with suspected intra-articular hip injury revealed uncommon injury patterns which we hypothesize is from a mechanism consistent with axial loading of the flexed knee in various degrees of hip flexion. Osseous, cartilaginous, and labral pathology were widely distributed throughout the joint particularly involving the posterior labrum and acetabulum. Although rare, serious complications may occur. Increased awareness of these injuries will aid physicians in interpretation and prompt diagnosis and treatment.
Declarations
Human subjects: Consent was obtained or waived by all participants in this study. University of Missouri Institutional Review Board issued approval 2004777.
Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue.
Conflicts of interest: In compliance with the ICM]E uniform disclosure form, all authors declare the following:
Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work.
Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work.
Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
References
- Agten CA, Sutter R, Buck FM, Pfirrmann CWA. Hip Imaging in Athletes: Sports Imaging Series. Radiology. 2016; 280: 351-369. 10.1148/RADIOL.2016151348
- Bodendorfer BM, Alter TD, DeFroda SF, et al. Multicenter Outcomes After Hip Arthroscopy: Comparative Analysis of Patients Undergoing Concomitant Labral Repair and Ligamentum Teres Debridement Versus Isolated Labral Repair. Orthop J Sports Med. 2021; 9. 10.1177/23259671211036469
- Byrd JWT, Jones KS. Traumatic rupture of the ligamentum teres as a source of hip pain. Arthroscopy. 2004; 20: 385-391. 10.1016/J.ARTHR0.2004.01.025
- Dangin A, Tardy N, Wettstein M, May O, Bonin N. Microinstability of the hip: A review. Orthop Traumatol Surg Res. 2016; 102: 301-309. 10.1016/J.OTSR.2016.09.002
- de Sa D, Hölmich P, Phillips M, et al.: Athletic groin pain: A systematic review of surgical diagnoses, investigations and treatment. Br J Sports Med. 2016; 50: 1181-1186. 10.1136/BJSPORTS-2015-095137
- Domb BG, Jackson TJ, Carter CC, Jester JR, Finch NA, et al. Magnetic Resonance Imaging Findings in the Symptomatic Hips of Younger Retired National Football League Players. Am J Sports Med. 2014; 42: 1704-1709. 10.1177/0363546514531551
- Drakos M, Domb B, Starkey C, Callahan L, Allen A. Injury in the national basketball association: A 17-year overview. Sports Health. 2010; 2: 284-290. 10.1177/1941738109357303
- Feeley BT, Powell JW, Muller MS, Barnes RP, Warren RF, et al. Hip Injuries and Labral Tears in the National Football League. The. American Journal of Sports Medicine. 2008; 36: 2187-2195. 10.1177/0363546508319898
- Groh MM, Herrera J. A comprehensive review of hip labral tears. Curr Rev Musculoskelet Med. 2009; 2: 105-117. 10.1007/S12178-009-9052-9
- Hua KC, Yang XG, Feng JT, Wang F, Yang L, et al. The efficacy and safety of core decompression for the treatment of femoral head necrosis: a systematic review and meta-analysis. J Orthop Surg Res. 2019; 11: 306. 10.1186/513018-019-1359-7
- Jonasson P, Halldin K, Karlsson J, et al. Prevalence of joint-related pain in the extremities and spine in five groups of top athletes. Knee Surg Sports Traumatol Arthrosc. 2011; 19: 1540-1546. 10.1007/S00167-011-1539-4
- Khanna V, Harris A, Farrokhyar F, Choudur HN, Wong IH. Hip arthroscopy: Prevalence of intra-articular pathologic findings after traumatic injury of the hip. Arthroscopy. 2014; 30: 299-304. 10.1016/J.ARTHRO.2013.11.027
- Knapik DM, Farivar D, Kunze KN, Gilat R, Nho SJ, et al. Indications and Outcomes After Ligamentum Teres Reconstruction: A Systematic Review. Arthrosc Sports Med Rehabil. 2021; 3: 939-949. 10.1016/J.ASMR.2021.01.023
- Makovicka JL, Chhabra A, Patel KA, Tummala SV, et al. A Decade of Hip Injuries in National Collegiate Athletic Association Football Players: An Epidemiologic Study Using National Collegiate Athletic Association Surveillance Data. Journal of Athletic Training. 2019; 54: 483. 10.4085/1062-6050-59-18
- McCarthy J, Noble P, Aluisio F V, Schuck M, Wright I, et al. Anatomy, pathologic features, and treatment of acetabular labral tears. Clin Orthop Relat Res. 2003; 38: 47. 10.1097/01.BLO.0000043042.84315.17
- Moorman CT, Warren RF, Hershman EB, et al. Traumatic posterior hip subluxation in American football. J Bone Joint Surg Am. 2003; 85: 1190-1196. 10.2106/00004623200307000-00002
- Nazareth A, Cooper B, Hollenbeck SM. Traumatic Posterior Hip Dislocation and Epiphysiolysis in a High School Football Player with Successful Outcome at 4 Years Follow-up: A Case Report. JBJS Case Connect. 2020; 10. 10.2106/JBJS.CC.20.00104
- Pallia CS, Scott RE, Chao DJ. Traumatic hip dislocation in athletes. Curr Sports Med Rep. 2002; 1: 338-345. 10.1249/00149619-200212000-00007
- Rao J, Zhou YX, Villar RN. Injury to the ligamentum teres. Mechanism, findings, and results of treatment. Clin Sports Med. 2001; 20: 791-800. 10.1016/S02785919(05\70285-4
- Safford DW, Pontillo M, Sennett BJ. Traumatic Hip Dislocation in an NCAA DI Football Player with Occult Sequelae: A Case Report. Int J Sports Phys Ther. 2021; 16. 10.26603/001C.28229
- Shapira J, Yelton MJ, Rosinsky PJ, et al. Ligamentum Teres Reconstruction May Lead to Improvement in Outcomes Following a Secondary Hip Arthroscopy for Symptomatic Microinstability: A Systematic Review. Arthroscopy. 2021; 37: 1811-1819. 10.1016/J.ARTHRO.2021.01.022
- Tibor LM, Sekiya JK. Differential diagnosis of pain around the hip joint. Arthroscopy. 2008; 24: 1407-1421. 10.1016/J.ARTHRO.2008.06.019
- Werner J, Hägglund M, Waldén M, Ekstrand J. UEFA injury study: a prospective study of hip and groin injuries in professional football over seven consecutive seasons. Br J Sports Med. 2009; 43: 1036-1040. 10.1136/BJSM.2009.066944
- Woodward RM, Vesey RM, Bacon CJ, White SG, Brick MJ, et al. Microinstability of the hip: A systematic review of the imaging findings. Skeletal Radio. 2020; 49: 1903-1919. 10.1007/S00256-020-03516-7