Introduction
Traumatic brain injury can lead to persistent cognitive, neurobehavioral, intellectual, academic, and personality problems in children [1]. Even mild traumatic brain injury may lead to persistent cognitive and behavioral deficits [1]. Injury severity is a strong predictor of long-term outcomes, with environmental factors playing a less consistent role [2]. Survivors of TBI are particularly vulnerable, with impairments that can impact on school performances, quality of life, and mental health [2]. Even though majority of children with TBI do have good functional recovery, a relatively high proportion (43%) of children with TBI develop disabilities that may interfere with their daily lives, such as temper outbursts, mood swings, memory problems, and learning difficulties [1,2]. It has been postulated that minor residual deficits are potentially more destructive to children than to adults with consequences that may interfere with schoolwork and social functioning [3]. Cognitive and behavioral problems are frequently reported by patients even several years post-injury [4]. This finding is consistent with that of other investigators [5,6]. Patients who had TBI more often report feeling sad or depress compared to people without history of TBI [7,8]. It is observed that subclinical executive problems are commonly experienced by individuals who had TBI and this may add to the total symptom burden [8]. However, in many instances problem-solving and task monitoring were not perceived as problematic among patients who had TBI [8]. This is in contrast to a study comprising moderate and severe TBI survivors, where these functions were perceived as most problematic [9]. The development of behavior problems can be affected by numerous factors including academic failure, vulnerability related to the environment, pre-injury characteristics such as communication difficulties, post-injury interventions or expectations, social relationships and family relationships [10]. Studies have found an associations between behavioral problems following TBI and school performance, intellectual ability, social deprivation and parental marital status [10]. Behavioral problems after TBI have also been linked with pre-injury behavioral and family functioning by several studies. It is likely, therefore, that social deprivation and parental separation are risk factors for behavioral problems after traumatic brain injury [11]. Children with behavioral problems disrupt not only their own education, but also that of their classmates [11]. Consequently, it is important that children at risk of these problems are identified and supported [11].
Objective
To study the impact of traumatic brain injury on children’s psychomotor and neurocognitive wellbeing.
Patients/methods
Study design: This is a retrospective/prospective cohort study involving all children aged 0 to 9 years admitted into UCTH with traumatic brain injury between January, 2016 and December, 2020.
Data collection: Patients’ hospital records were studied to retrospectively obtain clinic-demographic data to include age, sex, education before trauma, aetiology, admitting GCS, type of management (operative versus non-operative) and GCS at discharge. Prospective data was obtained using current clinical state, current educational attainment, type of school and presence or absence of independent life to determine outcome measures.
Ethical considerations: This study was carried out after ethical approval from the University of Calabar Ethics and Research Committee.
Consent: Informed consent for inclusion into the study was obtained using consent form in Appendix I. The nature of the study was carefully explained to patients if they are above 16 years of age or Gillick competent at the time of recruitment into the study or from their parents/caregivers if less than 16 years of age.
Confidentiality: Patients’ privacies were respected and treated with strict confidentiality.
Inclusion criteria: All patients treated for childhood traumatic brain injury (between the ages ≤1 to 9 years) at the University of Calabar Teaching Hospital between January, 2016 and December, 2020 who are currently within the ages of 10 and 19 years were recruited into the study.
Exclusion criteria: All patients between the ages of 1 and 9 years who were treated for childhood traumatic brain injury at the University of Calabar Teaching Hospital between January, 2016 and December, 2020 who are currently above 19 years old were excluded from the study. All patients who were treated for childhood traumatic brain injury between January, 2018 and December, 2020 but died before the age of 10 years were excluded from the study. All patients with pre-existing neurological disease(s) were excluded from the study. Patients with spinal cord injuries were excluded from the study; Patients who did not do brain computed tomography were excluded.
Sample size: The sample size was calculated using the fisher’s formula as follows:
n = z2pq/d2
Allowing for an attrition rate of 10%, a minimum of 88 patients were recruited into the study.
Data management and analysis: Data was analyzed using statistical packages for the social sciences (IBM SPSS statistics for Windows, Version 21.0. Armonk, NY: IBM Corp.). Data collected on proformas (Appendices II, III and IV) was entered into the SPSS spreadsheet using numerical codes.
Results
For descriptive purposes, the current age of the patients was categorized into early adolescence (10-15) and late adolescence (16-19) respectively. Greater than seventy one percent {71.59% (63/88)} of the patients were in their early adolescence (age range of 10-15) while the remaining 28.41% (25/88) were in their late adolescence (age range of 16-19). The real age (absolute age) of the patients) was obtained in months with a mean and median age of 150.92±35.14 and 132 respectively (Tables 1 & 2).
Table 1: Age group distribution.
| Age category (Years) |
Frequency (n=88) |
Percentage (%) |
| Age at the time of study |
|
|
| 10-15 |
63 |
71.59 |
| 16-19 |
25 |
28.41 |
Table 2: The course of endoscopic treatments.
| Measure of central tendency |
Age at time of study (Months) |
| Mean ± SD |
150.92±35.14 |
| Median |
132.00 |
| Mode |
120.00 |
| Minimum |
108.00 |
| Maximum |
228.00 |
Fifty nine percent of the patients were male {59% (52/88)} while 41% (36/88) were females with male female ratio of 1.4. Figure 1.
The Glasgow Coma Score(GCS) was used in this study to measure the severity of injury at presentation and it was categorized into: GCS 3-8 (mild head injury), GCS 9-12 (moderate head injury) and GCS 13-15 (severe head injury) respectively. More than forty four percent {44.32% (39/88)} of the patients had GCS of 3-8 while 40.91% (37/88) and 13.64% (12/88) had GCS of 9-12 (moderate head injury) and GCS of 13-15 (severe head injury) respectively. The data for this study was obtained retrospectively, this precluded the measurement of Glasgow Outcome Scores (GOS or GOSE) and its use for treatment outcome. Therefore, for the purpose of this study the Glasgow Coma Score at the time of discharge was obtained and used as guide to outcome at the time of discharge from the hospital. The GCS at discharge from the hospital was 9-12 (moderate injury) for 1.14% (1/88) patient and 13-15 (mild injury) for 98.86% (87/88) patients respectively. However, no patient was discharge at a GCS of 3-8. The mean GCS at the time of trauma was 8.63 with a standard deviation of ±3 while the mean GCS at the time of discharge from the hospital after successful treatment was 14.58 with a standard deviation of ±0.7 (Tables 3A & 3B).
Table 3A: Classification of injury severity with GCS.
| GCS Category |
Frequency (n=88) |
Percentage (%) |
| At Presentation |
| 3-8 |
39 |
44.32 |
| 9-12 |
37 |
40.91 |
| 13-15 |
12 |
13.64 |
| At discharge |
| 9-12 |
1 |
1.14 |
| 13-15 |
87 |
98.86 |
Table 3B: Measure of central tency for GCS classification of injury.
| Measure of central tendency |
GCS at presentation |
GCS at discharge |
| Mean ± SD |
8.63±3.13 |
14.58±0.72 |
| Median |
9 |
15 |
Falls mostly from domestic accident was responsible for 39.77% (35/88) of the traumatic brain injury in our patients. Pedestrian road traffic accident was second most frequent aetiology and is responsible for 34.09% (30/88) of the traumatic head injury in our patient. The remaining 26.14% (23/88) of the patients had traumatic brain injury caused by vehicular passenger road traffic accident {5.68% (5/88)}, Motor Cycle road traffic accident {7.95% (7/88)}, bicycle fall {1.14% (1/88)}, assault {2.27% (2/88)} and sport injury {9.09% (8/88)} (Table 4).
Table 4: Aetiology.
| Aetiology |
Frequency (n=88) |
Percentage (%) |
| Fall |
35 |
39.77 |
| Pedestrian RTA |
30 |
34.09 |
| Vehicular Passenger RTA |
5 |
5.68 |
| Motor Cycle RTA |
7 |
7.95 |
| Bicycle fall |
1 |
1.14 |
| Assault |
2 |
2.27 |
| Sport |
8 |
9.09 |
Operative treatment was carried out in 20.45% (18/88) of the patients while the remaining 79.55% (70/88) patients had only non-operative treatment. More than eighteen percent {18.18% (16/88)} had blood transfusion in the course of treatment and equal number of patients {18.18% (16/88)} had Intensive Care Unit admission (Table 5).
Table 5: Management.
| Type of management |
Frequency (n=88) |
Percentage (%) |
| Treatment |
| Operative |
18 |
20.45 |
| Non-operative |
70 |
79.55 |
| Blood transfusion |
| Yes |
16 |
18.18 |
| No |
72 |
81.82 |
| ICU admission |
| Yes |
16 |
18.18 |
| No |
72 |
81.82 |
Many of the patients {35.23% (31/88) had not started school at the time of the injury. Conversely, only 5.65% (5/88) of the patients were not schooling after discharge from the hospita and at the time of this study. More than sixty one percent {61.36 (54/88)} of the patients were in nursery or primary schools while only 3.41% (3/88) were in secondary school before the injury occurred. However, after treatment and at the time of this study, 48.86% (43/88) were still in primary school while 43.18% (38/88) were in secondary school. Expectantly, no patient had started post-secondary or tertiary level of education before the time of trauma but at the time of this study, 2.27% (2/88) of the patients were already in the University.
Among 64.77% (57/88) patients who started school before the time of trauma, none had poor or average performance grade in school while 50.88% (29/57) and 49.12% (28/57) had good performance and excellent performance grades in their last pre- injury academic session reports respectively.
Post-injury, 94.31% (83/88) of the patients were now in school while 5.68% (5/88) where not yet in school. Academic progress report after trauma was also obtained and last post-injury academic report prior to the time of this study showed that among the patients who were in school post- injury. 7.23% (6/83) had poor performance grade, 19.28% (16/88) had average performance grade, 40.96% (34/83) had good performance grade and 32.53% (27/83) had excellent performance grade (Table 6).
Table 6: School attendance and performance.
| Education level |
Before injury (%) |
After injury (%) |
| None |
31(35.23) |
5(5.68) |
| Nursery/Primary |
54(61.36) |
43(48.86) |
| Secondary |
3(3.41) |
38(43.18) |
| Post-secondary |
0(0.00) |
2(2.27) |
| Total |
88(100.00) |
88(100.00) |
| Performance in School |
| Poor |
0(0.00) |
6(6.82) |
| Average |
0(0.00) |
16(18.18) |
| Good |
29(32.95) |
34(38.64) |
| Excellent |
28(31.82) |
27(30.68) |
| None |
31(35.23) |
5(5.68) |
| Total |
88(100.00) |
88(100.00) |
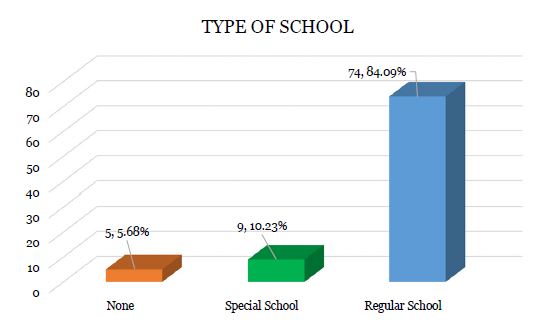
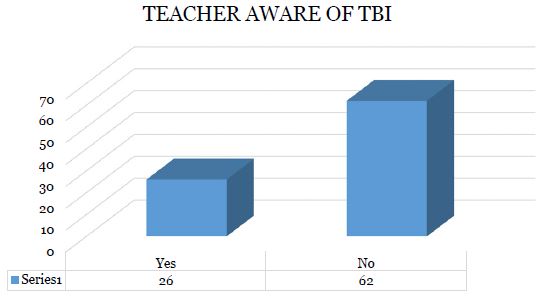
Among the 94.31% (83/88) of the patients who were schooling at the time of this study, 10.84% (9/83) were into special education while 89.16% (74/83) were in regular schools. In 29.55% (26/88) of the patients the teachers and/or schools were not informed of the head injury. However, in 70.45% (62/88) of the patients the teachers and/or the school authorities were informed (Figures 2 & 3).
More than twenty six percent {26.14% (23/88)} of the patients had some form of dependence in daily activities while 73.86% (65/88) had no dependence. Grade I (Moderate Dependence) was seen in majority of the patients who had dependence (21.59% (19/88) while grade II (Severe Dependence) and grade III (Major Dependence) accounted for 3.41% (3/88) and 1.14% (1/88) respectively (Table 7).
Table 7: Physical and social dependence.
| Dependent |
Frequency (n=88) |
Percentage (%) |
| Yes |
23 |
26.14 |
| No |
65 |
73.86 |
| Degree of Dependence |
| Grade 1 (Moderate dependence) |
19 |
21.59 |
| Grade 2 (Severe dependence) |
3 |
3.41 |
| Grade 3 (Major disability |
1 |
1.14 |
| No |
65 |
73.86 |
Some of the patients continued to have long term sequelae that are attributable to the traumatic brain injury even up to the period of this research. More than twenty two percent of the patients studied (22.73% (20/88) were still experiencing some form of headache. However, large number of patients {77.27% (68/88)} did not have headache. Twenty five percent (22/88) of the patients were still experiencing dizziness while 75% (66/88) had no dizziness. Neuro-behavioral problems were quite prevalent in most of the patients: Mood swing was being experienced by 18.18% (16/88) of the patients while the remaining 81.82% (72/88) had no mood abnormality. Half of the patients {50% (44/88)} do experience sleep abnormalities such as recurrent nightmares. However, equal number of patients (50% (44/88) do not experience any sleep abmormality. Aggressive behaviours were noticed in 10.23% (9/88) of the patients compare to the large subset of patients without aggressive behavioral problems. Other than aggressive behaviours, 12.50% (11/88) of the patients had other forms of inappropriate behaviours. Above seventeen percent {17.05% (15/88)} of the patients had depression compared with 82.95% (73/88) without depression. Most of the patients were still experiencing some motor dis orders that are characterized by clumsiness {22.73% 20/88)}, quick tiredness {14.77% (13/88)} and balance and coordination problems {19.32% (17/88)}. Large number of patients also developed various forms of language disorders characterized by receptive language deficit {14.77% (13/88)}, expressive language deficit {19.32% (17/88)}, and word finding difficulty {46.59% (41/88). Cognitive problems such as attention deficit {31.82% (28/88) and memory problems {28.41% (25/88) were also noticed in some patients Table 8.
Table 8: Long term clinical sequelae.
| Clinical Features |
Frequency (n=88) |
Percentage (%) |
| Headache |
| Yes |
20 |
22.73 |
| No |
68 |
77.27 |
| Dizziness |
| Yes |
22 |
25.00 |
| No |
66 |
75.00 |
| Mood swing |
| Yes |
16 |
18.18 |
| No |
72 |
81.82 |
| Anxiety |
| Yes |
12 |
13.64 |
| No |
76 |
86.36 |
| Nightmares |
| Yes |
44 |
50.00 |
| No |
44 |
50.00 |
| Aggressive behaviours |
| Yes |
9 |
10.23 |
| No |
79 |
89.77 |
| Feels down(depressed) |
| Yes |
15 |
17.05 |
| No |
73 |
82.95 |
| Clumsiness |
| Yes |
20 |
22.73 |
| No |
68 |
77.27 |
| Tiredness |
| Yes |
13 |
14.77 |
| No |
75 |
85.23 |
| Balane and Coordination problem |
| Yes |
17 |
19.32 |
| No |
71 |
80.68 |
| Receptive language deficit |
| Yes |
13 |
14.77 |
| No |
75 |
85.23 |
| Word finding difficulty |
| Yes |
41 |
46.59 |
| No |
47 |
53.41 |
| Expressive language deficit |
| Yes |
17 |
19.32 |
| No |
71 |
80.68 |
| Attention Deficit |
| Yes |
28 |
31.82 |
| No |
60 |
68.18 |
| Memorydisorder |
| Yes |
25 |
28.41 |
| No |
63 |
71.59 |
| Inappropriate behaviour |
| Yes |
11 |
12.50 |
| No |
77 |
87.50 |
Discussion
Changes initiated by traumatic brain injury can persist for years and significantly affect quality-of-life [12]. Chronic Post-Traumatic Headache (CPTHA), is one of the most frequent complaints following recovery from traumatic brain injury which could affect quality of life and function with a prevalence of 47-95% [13]. However, only 22.73% of our patients had chronic post-traumatic headache, this is relatively lower compared to the literature above. Chronic post-traumatic headache is often associated with dizziness and lack of concentration [13]. In our study 25% of our patients had dizziness while attention deficit was found in 31.82%. Mood disorder is commonly seen among patients treated for traumatic brain trauma [14]. A nationwide population-based study showed 2.97% of the patients treated for traumatic brain injury had a diagnosis of mood disorders in the 5-year follow-up period compared to 1.52% without antecedent traumatic brain injury [14]. In comparison our results showed higher frequency of mood abnormality in the form of mood swing (18.18%). Sleep disturbance is common following Traumatic Brain Injury (TBI), affecting 30-70% of individuals [15]. Traumatic brain injury triggers parasomnias, including sleepwalking, sleep terrors, REM sleep behavior disorder and dissociative disorders [16,17]. The most common sleep disorder experienced by our patients was nightmares seen in 50% of the cases. Challenging behaviours are serious chronic sequelae after a moderate-to-severe traumatic brain injury [18]. Defined as deviance from socio-cultural or developmental norms [18]. These behaviours may present barriers to community participation and risks to individual and caregivers’ health and safety, thereby undermining dignity and quality of life [18-20]. More than half of survivors will exhibit challenging behaviours in the first two-years post-TBI [18]. The most common being aggressive behavious socially inappropriate behaviours (e.g., standing too close to strangers, excessive apologising, failing to pick up nonverbal clues), and apathy [18]. In our study we observed Aggressive behaviors in 10.23% of the patients while inappropriate anti-social behaviors were seen in 12.50% of the patients. Higher level of aggression and antisocial behavior have been found in the period following head trauma [21,22]. These changes are attributable to specific brain alterations that generally involved frontal lobe, insula and limbic system [22].
More than seventeen percent (17.05%) of the patients studied had depression. Depression is a common sequelae of TBI with about 56% of individuals having symptoms of depression within one year post-injury [23]. Following a moderate-to-severe injury, the cumulative rate of major depressive disorder during the first year was found to be 53%, compared to the rate of major depressive disorder in the general population which is around 7% [24].
Traumatic brain injury is now known to be a chronic disease [25]. Traumatic brain injury is a cause of ongoing neurodegeneration and linked to increased risk of neurodegenerative motor diseases, such as Parkinson’s disease and amyotrophic lateral sclerosis [25]. Both traumatic and acquired brain injury can result in diffuse multifocal injury affecting both the pyramidal and extrapyramidal tracts [26]. Following traumatic brain injury, patients may exhibit signs of both upper motor neuron syndrome and movement disorder simultaneously which can further complicate diagnosis and management [26]. Tremor and dystonia are the most reported movement disorders following traumatic brain injury [26]. However, clumsiness (22.73%,), quick tiredness (14.77%) and balance and coordination problems (19.32%) were the major motor disorders experienced by the patients in this study. TBI can cause damage to language-based cognition [27]. This was found in a study with a higher risk of brain injured young people not achieving language-associated National Assessment Program-Literacy and Numeracy (NAPLAN) assessments compared to their matched counterparts [27-29]. Significant number of patients in this study developed various form of language disorders characterized by receptive language deficit (14.77%), expressive language deficit (19.32%) and word finding difficulty (46.59%) that can affect their learning abilities.
TBI is known to be associated with a decline in academic capacity and school performance [30]. Previous study has shown that children with brain injury were significantly disadvantaged compared to controls in terms of information processing and classroom performance [31]. This study also reported that teachers were particularly concerned about memory and attention deficits [31]. It has also been reported that children who under-achieve at school are often those who are easily distractible [32,33]. In our study, 28.41% of the patients had problem with memory and 31.82% had complaint of attention deficit that is keenly observed by the parents and adjudged to be the cause of current poors academic performance. This study has shown an improvement in school enrolment rate after discharge from the hospital when compared with pre-injury school enrolment: Before sustaining traumatic brain injury, 40.91% of our patients were not enrolled in school whereas only 9.09% were not enrolled in school after treatment. This improvement in enrolment rate was partly due to the fact that majority of the patients (56.82%) were within the pre-school age group prior to the injury. Previous study showed that for children with TBI, a return to mainstream regular schools is associated with good recovery [32,33]. However, the classroom environment, typically with one teacher to ~30 pupils, is likely to place a child who had traumatic brain injury at a disadvantage because majority of them are less able to focus and sustain attention [34]. Children who return to school after a TBI may therefore have residual cognitive and behavioural deficits which can prevent them from performing at previous educational levels [34]. This is congruous with the finding in this study I which none of the patients had poor or average school performance prior to injury whereas following resumption in school after treatment for traumatic brain injury, 6.82% and 18.18% of the patients started having poor and average school performance respectively.
Paediatric brain injury is under identified within school setting [35]. Under-identification of paediatric brain injury is partly because of ineffective communication between medical personals and educational institutions as youths return to school [35]. Teachers, parents, and clinicians often fail to link academic challenge to previous traumatic brain injury [36]. These assertions are further corroborated by our finding in which 70.45% of the patients studied, either the teachers nor the school authorities were informed about the history of the child’s traumatic brain injury. Teachers are rarely conversant with possible long-term effects of TBI, and many felt that as the TBI had been some years ago, they did not consider the child’s current school performance to be related to the injury [36]. Consequently, even when teachers know about the TBI, allowances were not routinely made for the possible effects of that injury. Some investigators concluded that there is inadequate educational provision for children after brain injury, mainly due to inaccurate or poor information for schools, poor communication between schools and hospitals, and inadequate training of teaching staff into the effects of TBI [37].
Declarations
Ethics approval and consent to participate: Ethical approval was granted by the Institution’s Ethical and Research Committee
Consent for publication: Not applicable
Availability of data and material: The dataset and materials used for this study are available from the corresponding author on reasonable request.
Competing interests: None.
Funding: The authors received no external funding for the study design; data collection, analysis and interpretation; or for writing the manuscript.
Authors’ contributions: All authors contributed to the research idea and methodology. O.H. collected, analyzed, and interpreted the data. O.H. completed the first draft of the article. J.A. and K.A. contributed to drafting and revising the manuscript. All authors read and approved the final manuscript.
Acknowledgements: Not applicable.
References
- CA Hawley, AB Ward, AR Magnay, J Long. Outcomes following childhood head injury: a population Study. J Neurol Neurosurg Psychiatry. 2004; 75: 737-742. doi: 10.1136/jnnp.2003.020651.
- Anderson Vicki, Brown Sandra, Newitt Heidi, Haile Hannah. Educational, Vocational, Psychosocial, and Quality-of-Life Outcomes for Adult Survivors of Childhood Traumatic Brain Injury. Journal of Head Trauma Rehabilitation. 2009; 24 (5): 303-312. doi:10.1097/HTR.0b013e3181ada830.
- Crouchman M, Rossiter L, Colaco T, et al. A practical outcome scale for paediatric head injury. Arch Dis Child 2001; 84:120–4.
- Thornhill S, Teasdale GM, Murray GD, McEwen J, Roy CW, Penny KI. Disability in young people and adults one year after head injury: prospective cohort study. BMJ. 2000; 320: 1631
- Chadwick O, Rutter M, Brown G, et al. A prospective study of children with head injuries: II. Cognitive sequelae. Psychol Med. 1981; 11: 49-61.
- Scott-Jupp R, Marlow N, Seddon N, et al. Rehabilitation and outcome after severe head injury. Arch Dis Childhood. 1992; 67: 222-6.
- Donders J, Ballard E. Psychological adjustment characteristics of children before and after moderate to severe traumatic brain injury. J Head Trauma Rehabil. 1996; 11: 67-73.
- Guyer B, Ellers B. Childhood injuries in the United States. Am J Dis Child. 1990; 144: 649-52.
- A Garc´ıa-Molina, JM Tormos, M Bernabeu, C Junqu´e, T Roig-Rovira. Do traditional executive measures tell us anything about daily-life functioning after traumatic brain injury in Spanish-speaking individuals? Brain Injury. 2012; 26(6): 864-874.
- MJ Rapoport. Depression following traumatic brain injury: Epidemiology, risk factors and management. CNS Drugs. 2012; 26(2): 111-121.
- Corso P, Finkelstein E, Miller T, Fiebelkorn I, Zaloshnja E. Incidence and lifetime costs of injuries in the United States. Inj Prev. 2006; 12(4): 212-218.
- Schwartz L, Taylor HG, Drotar D, Yeates KO, Wade SL, et al. Long-term behavior problems following pediatric traumatic brain injury: Prevalence, predictors, and correlates. J. Pediatr. Psychol. 2003; 28: 251-263.
- Sumpter R, Brunklaus A, McWilliam R, Dorris L. Health-related quality-of-life and behavioral outcome in survivors of childhood meningitis. Brain Inj. 2011; 25: 1288-1295.
- Meng-Che Tsai, Kuen-Jer Tsai, Hao-Kuang Wang, Pi-Shan Sung, Ming-Hsiu Wu, et al. Mood Disorders after Traumatic Brain Injury in Adolescents and Young Adults: A Nationwide Population-Based Cohort Study. The Journal of Pediatrics. 2014; 164(1): 136-141.e1. https://doi.org/10.1016/j.jpeds.2013.08.042.
- Wolfe LF, Sahni AS, Attarian H. Sleep disorders in traumatic brain injury. Neurorehabilitation. 2018; 43: 257-266.
- Viola-Saltzman M, Watson NF. Traumatic brain injury and sleep disorders. Neurol Clin. 2012; 30(4): 1299-1312. doi:10.1016/j.ncl.2012.08.008
- Maresca G, Lo Buono V, Anselmo A, et al. Traumatic Brain Injury and Related Antisocial Behavioral Outcomes: A Systematic Review. Medicina (Kaunas). 2023; 59(8): 1377. Published 2023 Jul 27. doi:10.3390/medicina59081377.
- Hendryckx C, Nalder E, Drake E, et al. Managing challenging behaviours in adults with traumatic brain injury: A scoping review of technology-based interventions. J Rehabil Assist Technol Eng. 2023; 10: 20556683231191975. Published 2023 Aug 21. doi:10.1177/20556683231191975.
- Emerson E, Bromley J. The form and function of challenging behaviours. J Intellect Disabil Res. 1995; 39(5): 388-398.
- Mc Villy KR, Bristow S, Foreman P, et al. Positive behaviour support for people with intellectual disability: Evidence-based practice, promoting quality of life. Australian Society for the Study of Intellectual Disability. 2002.
- Tassé MJ, Sabourin G, Garcin N, et al. Définition d’un trouble grave du comportement chez les personnes ayant une déficience intellectuelle. Canadian Journal of Behavioural Science/Revue canadienne des sciences du comportement 2010; 42(1): 62-69.
- Schenck CH, Boyd JL, Mahowald MW. A parasomnia overlap disorder involving sleepwalking, sleep terrors, and REM sleep behavior disorder in 33 polysomnographically confirmed cases. Sleep. 1997; 20(11): 972-81.
- Singh R, Mason S, Lecky F, Dawson J. Prevalence of depression after TBI in a prospective cohort: The SHEFBIT study. Brain Inj. 2018; 32: 84-90.
- Bombardier CH, Fann JR, Temkin NR, Esselman PC, Barber J, et al. Rates of major depressive disorder and clinical outcomes following traumatic brain injury. JAMA. 2010; 303: 1938-1945.
- Corrigan F, Wee IC, Collins-Praino LE. Chronic motor performance following different traumatic brain injury severity-A systematic review. Front Neurol. 2023; 14: 1180353. Published 2023 May 11. doi:10.3389/fneur.2023.1180353.
- Moon D. Disorders of Movement due to Acquired and Traumatic Brain Injury. Curr Phys Med Rehabil Rep. 2022; 10(4): 311-323. doi:10.1007/s40141-022-00368-1
- Jimenez N, Symons RG, Wang J, Ebel BH, Valvilala MS, et al. Outpatient rehabilitation for medicaid-insured children hospitalized with traumatic brain injury. Pediatrics. 2016; 137(6): e20153500.
- Glang A, Tyler J, Pearson S, Todis B, Morvant M. Improving educational services for students with TBI through statewide consulting teams. Neuro Rehabilitation. 2004; 19(3): 219-231.
- Glang A, Todis B, Thomas CW, Hood D, Bedell G, et al. Return to school following childhood TBI: who gets services? NeuroRehabilitation. 2008; 23(6): 477-486.
- Edwards SGM, Playford ED, Hobart JC, Thompson AJ. Comparison of physician outcome measures and patients’ perception of benefits of inpatient neurorehabilitation. BMJ. 2002; 324: 1493.
- Wood RL. Recognising and assessing neurobehavioural disability after traumatic brain injury. NeuroRehabilitation. 2013; 32(4): 699-706.
- Jimenez N, Ebel BE, Wang J, Koepsell T, Jaffe K, et al. Disparities in disability after traumatic brain injury among Hispanic children and adolescents. Pediatrics. 2013; 131(6): e1850-e1856.
- US Department of Education. IDEA section 618 data products: Static files. Available at: https://www2.ed.gov/programs/osepidea/618-data/static-tables/index.html.
- Gándara P, Rumberger R, Maxwell-Jolly J, Callahan R. English learners in California schools: Unequal resources, unequal outcomes. Educ Policy Anal Arch. 2003; 11(36). Available at: https://epaa.asu.edu/ojs/article/viewFile/264/390.
- Roscigno CI, Fleig DK, Knafl KA. Parent management of the school reintegration needs of children and youth following moderate or severe traumatic brain injury. Disabil Rehabil. 2015; 37(6): 523-533.
- Adeleye AO, Odero W, Garner P, Zwi A. Road traffic injuries in developing countries: A comprehensive review of epidemiological studies. Trop Med Int Health. 1997; 2: 445-460.
- Anderson V, Brown S, Newitt H, Hoile H. Long-term outcome from childhood traumatic brain injury: intellectual ability, personality, and quality of life. Neuropsychology. 2011; 25: 176.