Case
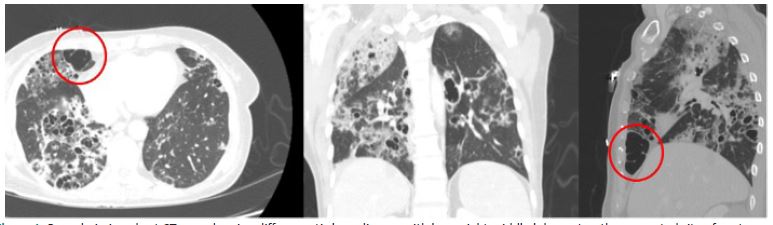
A 59-year-old woman with a history of HIV was admitted to an outside hospital for almost a month for workup of shortness of breath, hypoxia, and fevers. She had acute hypoxic respiratory failure due to PJP complicated by a large spontaneous right pneumothorax, which was first managed non-operatively with a pigtail catheter. She had a persistent pneumothorax with a large air leak despite placement of the chest tube on suction, raising concern for a Bronchopleural Fistula (BPF). Thoracic surgery was initially consulted at the outside facility for surgical management of the BPF; however, the patient was deemed not a candidate for pleurodesis or VATS intervention due to the high mortality risk associated with patients with a pneumothorax secondary to PJP. She was transferred to our facility for consideration of Endobronchial Valve (EBV) placement by Interventional Pulmonology for management of the BPF. However, during the bronchoscopy it was discovered that her anatomy was not amenable to the placement of EBVs as Interventional Pulmonology was unable to isolate the locus of the BPF. Thoracic surgery was consulted for surgical management. On exam, she had a large air leak from the chest tube. Imaging was notable for diffuse cystic lung disease with a large right middle lobe cyst, which was the suspected rupture site (Figure 1). The decision was made to go to the operating room for robot-assisted wedge resection and pleurodesis. Intraoperative findings were significant for dense fibrotic cystic lung disease with firm nodules and the large, ruptured cyst on the medial inferior portion of the right middle lobe as the site of the fistula (Figure 2). The cyst was resected with a stapler. A submersion leak test was performed, which was negative for leaks, and mechanical and chemical pleurodesis were completed. Please see the attached video of the operation. A chest tube was placed at the end of the case, which was removed 72 hours later without evidence of reaccumulation of the pneumothorax. The remainder of the hospital stay was uncomplicated.
Comment
The opportunistic infection pneumocystis jirovecii is the leading cause of secondary pneumothoraces in patients with HIV with an incidence around 35% [1-3]. The subset of patients with spontaneous pneumothoraces with HIV and PJP were more difficult to treat and had worse outcomes than patients with spontaneous pneumothoraces and HIV without PJP [2,4]. Ingram et al reports 50% mortality in patients with pneumothorax and PJP compared to 25% in patients who did not have PJP [2].
The pathogenesis is postulated to be secondary to rupture of subpleural cavities due to cystic lung disease and emphysematous blebs from the underlying infection, which makes the lung parenchyma friable and not amenable to traditional forms of therapy, as the lung will fail to expand leaving a persistent air leak [1,3-6]. Alveolar-pleural fistulas also develop as a complication of the infection, contributing to the reaccumulation of the pneumothorax after failed non-operative treatment attempts [6].
A stepwise approach is implemented to manage pneumothoraces in patients with HIV and PJP, starting with thoracostomy tubes and progressing to bedside pleurodesis and Heimlich valves, which requires a re-expanded lung for pleural apposition [1,2]. An additional form of treatment is EBVs, which is effective in patients who develop alveolo-pleural fistulas secondary to PJP [6]. It is important that the patient’s anatomy is amenable to this form of treatment. More invasive procedures such as VATS resection of blebs with pleurodesis, pleurectomy, and open surgical resection are also options [1,2]. Surgical intervention was the least utilized form of treatment in the literature with surgery performed in less than 3% of the cases [1,2].
Conclusion
Identifying patients with HIV and PJP who develop a pneumothorax is imperative due to the increased morbidity and mortality associated with the combination of these disease processes, in addition to the financial burden associated with utilization of resources to devise an effective treatment plan. This case reports highlights an underutilized treatment strategy for this select group of patients that will not only ameliorate the issue, but also decrease the cost burden associated with prolonged hospital stays. To our knowledge, we report the first case of robot-assisted resection and pleurodesis to manage this complex condition and have shown that it is a safe and effective option.
Declarations
Acknowledgements: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure/conflicts of interest: None.
References
- Terzi E, Zarogoulidis K, Kougioumtzi I, Dryllis G, Kioumis I, et al. Human immunodeficiency virus infection and pneumothorax. Journal of Thoracic Disease. 2014; 6(4): S377-S382. doi:10.3978/j.issn.2072-1439.2014.08.03
- Ingram RJH, Call S, Andrade A, White C, Wheeler D. Management and Outcome of Pneumothoraces in Patients Infected with Human Immunodeficiency Virus. Clinical Infectious Diseases. 1996; 23(3): 624-627. doi:10.1093/clinids/23.3.624
- Park YK, Jung HC, Kim SY, et al. Spontaneous Pneumomediastinum, Pneumopericardium, and Pneumothorax with Respiratory Failure in a Patient with AIDS and Pneumocystis jirovecii Pneumonia. Infect Chemother. 2014; 46(3): 204. doi:10.3947/ic.2014.46.3.204
- Afessa B. Pleural Effusion and Pneumothorax in Hospitalized Patients with HIV Infection. Chest. 2000; 117(4): 1031-1037. doi:10.1378/chest.117.1031
- Suwanwongse K, Shabarek N. Tension Pneumothorax Following Pneumocystis jirovecii Pneumonia. Cureus. 2020; 12(1): e6799. doi:10.7759/cureus.6799
- Vicencio AG, Tozzi M, Thompson C, et al. Intrabronchial valves for treatment of alveolar-pleural fistula in a patient with Pneumocystis jirovecii pneumonia. J Bronchology Interv Pulmonol. 2014; 21(4): 346-349. doi:10.1097/LBR.0000000000000104