Introduction
Although there is some risk intrinsic to participation in all recreational activities, the majority of sports-related injuries are minor. Admissions at trauma centers are most commonly due to motor-vehicle collisions, inter-personal violence, and falls; these mechanisms of injury also account for the highest mortality rates [1,2]. While certainly tragic and often of high-visibility due to media coverage, deaths and injuries requiring ICU admission due to sports appear to be rare.
We believe that if recreational activities involving motorized vehicles or firearms are excluded, then few sports-related injuries will result in death or require admission to a trauma center. We suspect that most injuries due to individual or team sports participation will occur in young men, will be minor and only comprise a small percentage of the trauma center admissions. We were to determine the incidence of sport-related injuries that require admission at a Trauma Center, and to describe this population of patients and the type of injuries sustained.
Methods
We conducted a retrospective review of the trauma registry of all admitted patients from 1995-2009. This registry is an electronic medical record that is maintained by specially trained nursing staff. The setting was an urban level-one trauma center located in an academic tertiary-care hospital. This trauma center receives patients 13 years of age and older. Included were individual and team sports and recreation activities such as roller-skating/roller-blading, basketball, football, baseball, tennis, wrestling, water skiing, and paintball games; excluded were motorized activities and sporting utilizing firearms (hunting, trap shooting, etc.).
Results
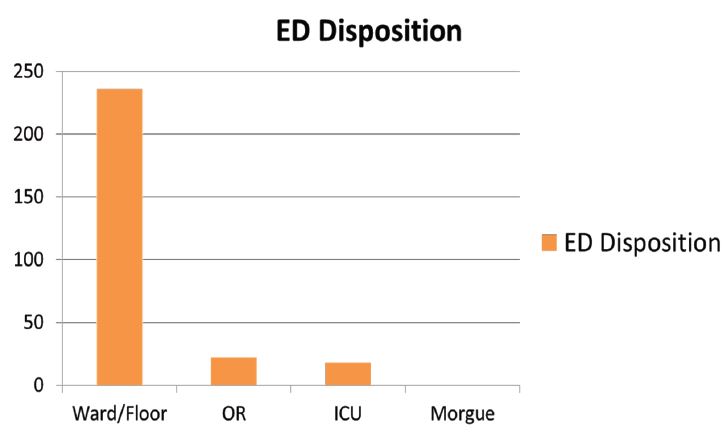
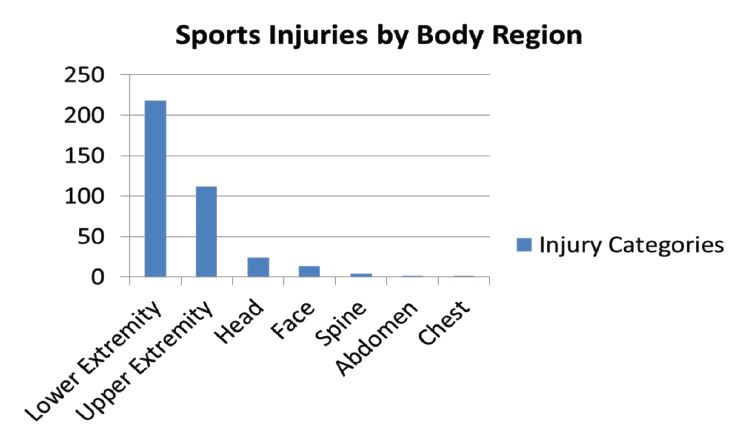
A total of 45,482 trauma patients were admitted during the study period, including 315 patients for sports-related injuries: 0.693% of all admissions. 276 were male (87.62%) and the average age was 27.02 years (range 13-58 years). 18 patients were admitted to the ICU and 22 patients we taken from the Emergency Department (ED) directly to the OR; there were no deaths (Figure 1). Injuries occurred to the following areas of the body: lower extremity (218), upper extremity (112), head (24), face (13), spine (4), abdomen (1) and chest (1) (Figure 2).
Limitations
Since our results are based on a retrospective analysis of an electronic data base, there are intrinsic flaws possible due to the nature of this type of database. We relied upon the appropriate coding of the injuries into specific categories of sports activities but there may have been some under-reporting specifically if an injury was not listed as due to a sport. We limited the sports activities to non-motorized, except for boats used in waterskiing, and no firearms; the involvement of motorized vehicles (ATV, dirt-bike, jet-ski, etc.) and guns would certainly increase the total number of injuries as well as the mortality rate.
Discussion
Each year in the U.S. approximately 30 million children and adolescents participate in organized sports while 150 million adults participate in non-work related physical activity [2]. In 2001, 4.3 million patients sought Emergency Department (ED) treatment for non-fatal sports and recreation related injuries in the U.S. with 2.3% of these patients requiring hospitalization [2]. The highest rates of sports and recreation related injuries occur in 10-14 year old boys while the lowest occur in women over 45 years old. Despite similar rates of participation in sports, males have a higher rate of injuries than females as well as more severe injuries thought to be due to differences in the nature of the activities and increased risk taking behavior [3,4].
Sports-related injuries are classified into direct and indirect, with the former being attributed to mechanical forces such as falls, collisions with other participants, or contact with equipment used in the activities while the latter includes heat related illness, dehydration and morbidity due to congenital diseases such as structural cardiac abnormalities, dysrhythmias, or sickle cell disease. Catastrophic sporting injuries, the most severe category, are further classified into Serious: severe in nature but without permanent disability such as a femur fracture or a splenic injury; Non-Fatal: severe with permanent disability such as a Spinal Cord Injury (SCI) with resultant deficit or a Traumatic Brain Injury (TBI) with cognitive impairment; and Fatal [1]. Football is still the sport with the highest number of catastrophic injuries despite the significant decrease in head and neck injuries since the 1976 rule change banning “spearing” or leading with the helmet during tackling [1,4]. Football also still leads as the sport with the highest rates of injuries during practice and competition, although the rate increases three-fold during games [4].
7% of the SCI and 10% of TBI leading to permanent disability occur due to sports and recreation related activities each year. The most commonly injured body parts are as such: ankle 12.1%, fingers 9.5%, face 9.2%, head 8.2%, and knees 8.1%; the most common types of injuries include: sprain/strain 29.1%, fracture 20.5%, contusion or abrasion 20.1%, and laceration 13.8% [2].
Conclusion
Non-motorized/non-firearm sports and recreational activities accounted for less than 1% of all trauma center admissions. There were no deaths and the majority of patients (87.31%) were admitted directly to a hospital floor. Orthopedic injuries to the lower and upper extremities were the predominant injury type, while young men were the most typical patients. Injury prevention strategies should focus on education of adolescent boys and young men, and protective equipment for the arms, legs, and head should be encouraged during sports.
Key messages
What is already known on this subject: Catastrophic injuries related to sports are fortunately uncommon.
What this study adds: A description of the population (young men and teenagers) who are at highest risk of sports-related injuries comprising mostly orthopedic injuries to their extremities but also face and head injuries.
How this study might affect research, practice or policy: Education prior to sports participation and use of appropriate equipment could reduce incidence and severity of these injuries.
Declarations
Disclosure statement: The authors report there are no competing interests to declare. This data was presented as a poster abstract at the IBIA Meeting 2012, Edinburgh Scotland.
Research ethics approval: study was reviewed by IRB and found to be Exempt.
References
- Gotsch K, Annest J, Holmgreen P, et al. Nonfatal sports and recreation related injuries treated in emergency departments, United States, July 2000- June 2001. JAMA. 2002; 288: 1977-8.
- Luckstead E, Patel D. Catastrophic pediatric sports injuries. Pediatr Clin North Am. 2002; 49: 581-91.
- Gabbe BJ, Finch CF, Cameron PA, et al. Incidence of serious injury and death during sport and recreational activities in Victoria, Australia. Br J Sports Med. 2005; 39: 573-77.
- American Association of Neurological Surgeons website: Patient Information Sports-Related Head Injury. www.aans.org/patient%information updated July 2010.