Introduction
In 2019, traumatic brain injuries were associated with approximately 223,135 hospitalizations [1]. Approximately 18-40% of head trauma injuries results in temporal bone fractures. The major cause is due to motor vehicle accidents, followed by falls and gunshot wounds. High-velocity head injuries carry the risk of significant morbidity and mortality because of injury to the cranial nerves or vasculature surrounding the bone structures. These patients frequently present with multiple lesions of varying severity. As a result, temporal fractures result in several complications including facial nerve palsy, cerebrospinal fluid leaks, and hearing loss.
Hearing loss is the most common chief complaint-occurring in as many as 40% of head trauma patients. It is usually apparent to the conscious patient immediately after the temporal bone trauma. The hearing loss may or may not result in tinnitus (ringing in the ears). Due to their location, temporal bone injuries often impact the cochlea and auditory nerve (CN VIII) potentially resulting in three types of hearing loss: conductive, sensorineural, and mixed hearing loss. Conductive hearing loss is dueto the injury to the conducting system distal to the cochlea and sensorineural results from injury to the internal ear including the cochlea and CV VIII. Mixed hearing loss is defined by partial injury to both set of structures. Typically, conductive, and mixed hearing loss are more common in longitudinal temporal bone fracture or injuries with no identifiable fracture, whereas sensorineural hearing loss is associated with transfer fractures. Audiometric testing can help differentiate between these types of hearing loss. Determining the type of hearing loss is prognostically important but does not influence the timing of surgery.
Hearing loss, especially mixed or profound, following temporal bone fractures have resulted in functional impairment. Profound hearing loss in one or both ears have been associated with lower Hearing Handicap Inventory (HHI), Tinnitus Handicap Inventory (THI), and Dizziness Handicap Inventory (DHI) values. The lower values display reduced functional abilities and social interaction of patients with post-temporal bone hearing loss. These impairments correspond to poor communication, depression, social withdrawal, and isolation. Although temporal bone fractures may not represent the patient’s acute threatening lesion, early involvement of an Otolaryngologist in initial assessment and management has potential to improve long-term functional results.
We performed a retrospective study on patients with temporal bone fractures who have had audiologic testing at Mercy Health Youngstown hospitals from December 1st, 2015, to December 1st, 2020. Our study objective is to follow the natural history of conductive and sensorineural hearing loss in patients with temporal bone fractures.
Materials and methods
IRB approval was obtained. Retrospective review of the trauma database of a regional institution, level 1 trauma center identifying patients diagnosed with temporal bone fracture from January 2015-January 2020 IRB approval was obtained. Retrospective review of the trauma database of a regional institution, level 1 trauma center identifying patients diagnosed with temporal bone fracture from January 2015-January 2020.
This retrospective cohort study consists of an analysis reviewing 79 patients with documented temporal bone fractures according to CT imaging from December 1, 2015 to December 1, 2020. All patients that are included in this review were treated at Mercy Health Youngstown hospitals (St Elizabeth Youngstown, St Elizabeth Boardman, and St Joseph’s). Only patients who underwent audiologic testing within 1 month of the initial injury were included. The patients reviewed were classified according to temporal bone fracture classification: longitudinal, transverse, or mixed. Demographic details, including age, ethnicity, gender, and additional comorbidities were included in the chart review. The course of their audiologic treatment and follow-up was documented, including initial audiograms, CT scan imaging, head and neck examinations, and follow-up audiologic testing. All recorded patient characteristics were manually entered into a separate spreadsheet for analysis.
Based on the classification by fracture type and demographic characteristics, the differences in audiologic morbidity between groups was compared. Statistical analysis included comparisons of mean, standard deviation and percent comparison based on different characteristics of temporal bone fracture.
Results
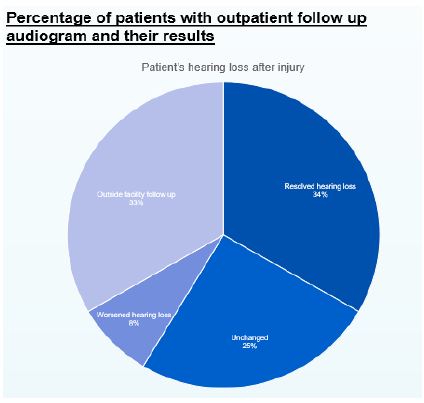
We performed a retrospective, single institution review of trauma patients that sustained skull base fractures from the years 2015 to 2020. A total of 2544 patients had skull base fractures and out of those, 79 patients were diagnosed with temporal bone fractures. The temporal bone fractures were analyzed based on side and orientation of fracture, mechanism of injury, age, type of hearing loss and intervention for hearing loss. The patients were 82% male, 91% Caucasian, and the age range was 11 years-96 years old (Table 1). The most common etiology was falls (29%) with motorcycle accidents as a close second (23%), as shown in Table 2. Patient’s sustained longitudinal, transverse or mixed temporal bone fractures with longitudinal making up the majority (50%) (Table 3). Fifty five percent of fractures occurred on the right side, followed by 33% on the left and 10% sustaining bilateral fractures (Table 4). Twenty-eight percent of patients had an initial audiogram performed once clinically stable, all but one showing some type of hearing loss. Fifteen percent (N=12) of patients followed up in the outpatient setting and out of those patients, the hearing loss outcomes were as follows: resolved (N=4), unchanged (N=3), worsened (N=1), patient followed with provider outside hospital system (N=4) (Figure 1). Two patients with hearing loss underwent intervention consisting of bone-anchored hearing aid or traditional hearing aid (Figure 2).
The patients that followed up in the outpatient setting with documented hearing loss were further analyzed. The majority of patients with outpatient follow up had right sided temporal bone fracture with longitudinal orientation. A motorcycle crash was the most common mechanism of injury associated with hearing loss. Out of the 15% of patients that followed in the outpatient setting, the most common type of hearing loss encountered was conductive hearing loss (62%) followed by mixed hearing loss (25%) (Table 5). The patient’s with resolved hearing loss all had initial conductive type hearing loss. Out of the two patients that underwent intervention for hearing loss, one patient had profound unilateral hearing loss and the other had bilateral moderate asymmetric mixed hearing loss, with a moderate to profound loss on the side of the temporal bone fracture side. Most patients with initial hearing loss after injury had resolution of their hearing loss at roughly 6 weeks after injury, not requiring intervention. Out of the patients with unchanged or worsening hearing loss, only 50% of those patients sought intervention as noted above.
Table 1: Age of Patient sustaining temporal bone fracture.
|
Age (years) |
| Youngest age |
11 |
| Oldest age |
96 |
| Average age |
46 |
| Median age |
49 |
Table 2: Mechanism of injury.
| Mechanism |
Number of patients (N) |
Percentage (%) |
| Fall |
23 |
29 |
| Motorcycle accident |
18 |
23 |
| ATV |
7 |
9 |
| Motor vehicle accident |
7 |
9 |
| Pedestrian vs MVA |
6 |
8 |
| Assault |
5 |
6 |
| Blow to head |
3 |
4 |
| Gunshot wound |
3 |
4 |
| Bicycle vs MVA |
3 |
4 |
| Bicycle accident |
1 |
1 |
| Horse accident |
1 |
1 |
| Seizure |
1 |
1 |
| Syncope |
1 |
1 |
Table 3: Orientation of temporal bone fracture.
| Orientation |
Number of patients (N) |
Percentage (%) |
| Longitudinal |
40 |
50 |
| Transverse |
10 |
13 |
| Mixed (oblique) |
14 |
18 |
| Unclassified |
15 |
19 |
Table 4: Side of temporal bone fracture.
| Fracture side |
Number of patients (N) |
Percentage (%) |
| Right |
45 |
57% |
| Left |
26 |
33% |
| Bilateral |
8 |
10% |
Table 5: Type of hearing loss sustained with temporal bone fracture.
| Type of hearing loss |
Percentage (%) |
| Conductive |
62% |
| Sensorineural |
0% |
| Mixed |
25% |
| Normal |
12.5% |
Discussion
It is widely known that temporal bone fractures can result in hearing loss. Due to the mechanism of injury to sustain a temporal bone fracture, patients typically present with polytrauma. It was our hypothesis that most patients did not undergo intervention for their hearing loss secondary to temporal bone fracture. We sought to evaluate temporal bone fractures, their associated hearing loss and the eventual need for intervention for hearing restoration.
The two most common serious consequences of traumatic temporal bone fractures are hearing loss and facial nerve paralysis [2,3]. Temporal bone trauma is usually the result of blunt head injury and patients commonly suffer from multiple other body injuries [2,3]. Previous studies have shown motor vehicle accidents are the most common cause, with falls and gunshot wounds contributing to a lesser extent [2,3]. In our retrospective review, falls were the most common cause of injury followed by motor vehicle accidents. Because the temporal bone encloses the middle and internal ear, these structures can be damaged by penetrating or concussive trauma to the tympanic membrane through the external acoustic meatus without temporal bone fracture [2]. This can result in a sensorineural hearing loss, conductive hearing loss or mixed hearing loss. We found conductive hearing loss being the most common type of hearing loss associated with temporal bone fracture. The majority of patients had longitudinally oriented temporal bone fracture (Table 3). Longitudinal temporal bone fractures are less likely to have otic capsule involvement and subsequently permanent hearing loss compared to transverse temporal bone fractures that more commonly involve the otic capsule [4]. Out of the patients who sought surgical hearing loss from their trauma, they suffered mixed type of hearing loss. Noting that most hearing loss was conductive in nature roughly 6 weeks after surgery and then improved. This indicates that hearing loss associated with temporal bone trauma is associated with hemotympanum and has a promising prognosis to resolve without much intervention [4-7].
The overwhelming majority of patients did not follow up for re-evaluation or hearing tests. This is thought to be due to several factors; the hearing loss improved spontaneously, patient was placed in a rehab facility and appointment was not arranged, other injuries prevailed as more significant. This study could have been improved if a greater number of patients followed up in clinic for serial audiograms. In trauma patients, it is difficult to obtain a pre-injury audiogram or audiogram at time of injury due to a multitude of factors including hemotympanum, brain injury, needs for sedation/ventilation, comorbidities. Therefore, the study is limited as a comparison between pre and post injury audiogram is not prevalent. For future studies, expanding the census of patients sustaining temporal bone fractures could increase the number of patients that could have potentially followed up to further analyze persistent hearing loss after temporal bone fracture.
In summary, conductive hearing loss was the most common type of hearing loss sustained. The patients that recovered their hearing had initial conductive hearing loss. Those patients that had sustained hearing loss most commonly had conductive hearing loss as well. Most patients with sustained hearing loss after injury had conductive hearing loss indicating temporal bone fracture hearing loss is likely related to ossicular discontinuity or potentially surgically fixable cause. An overwhelming majority of patients did not follow up for hearing evaluation. Causes of poor follow up could be related to the patient sustaining significant other injuries, placement in rehab or nursing facility preventing ease of office follow up, or subjective improvement of hearing. Those patients that did have prolonged follow up, only half underwent intervention.
While more clinical study is needed an assumption can be drawn that most patients with temporal bone fractures have subjective improvement of hearing not requiring intervention.
Conclusion
Our study population with temporal bone fractures had poor outpatient follow up. The majority of patients’ hearing improved with the minority undergoing hearing intervention. Most patients with sustained hearing loss after injury had conductive hearing loss indicating temporal bone fracture hearing loss is likely related to ossicular discontinuity or potentially surgically fixable cause. An overwhelming majority of patients did not follow up for hearing evaluation. Causes of poor follow up could be related to the patient sustaining significant other injuries, placement in rehab or nursing facility preventing ease of office follow up, subjective improvement of hearing. Those patients that did have prolonged follow up, only half underwent intervention. While more clinical study is needed an assumption can be drawn that most patients with temporal bone fractures have subjective improvement of hearing not requiring intervention.
Declarations
Conflicts of interest: There are no conflicts of interest to disclose.
Acknowledgements: None.
Funding: None.
References
- Antoniades E, Psillas G, Polyzoidis K, Patsalas I. Patient-Assessed Outcomes following Temporal Bone Fractures. Diagnostics. 2022; 12(2): p.547.
- Gunlock MG, Gentry LR. Anatomy of the temporal bone. Neuroimaging Clin N Am 1998; 8(1): 195-209.
- Proctor B. The anatomy of the facial nerve. Otolaryngol Clin North Am 1991; 24(3): 479-504.
- Patel A, Groppo E. Management of temporal bone trauma. Craniomaxillofac Trauma Reconstr. 2010; 3(2): 105-113. doi:10.1055/s-0030-1254383.
- Lyos AT, Marsh MA, Jenkins HA, Coker NJ. Progressive hearing loss after transverse temporal bone fracture. Arch Otolaryngol Head Neck Surg. 1995; 121(7): 795-9. doi:10.1001/archotol.1995.01890070081017. PMID: 7598860.
- Kamerer DB, Thompson SW. Middle ear and temporal bone trauma. In: Bailey BJ, ed. Head and Neck Surgery- Otolaryngology. 3rd ed. Philadelphia: Lippincott Williams & Wilkins. 2001.
- Bellucci RJ. Traumatic injuries of the middle ear. Otolaryngol Clin North Am 1983; 6(3): 633-650.