Introduction
ACTA2 (Actin, alpha 2) mutations are causative for familial thoracic aortic aneurysms and dissections. Especially, a specific ACTA2 missense mutation (Arg179His) leads to a distinctive, Multisystemic, Smooth Muscle Dysfunction Syndrome (MSDMS), including severe cerebrovascular disease [1], and high risk of surgical complications during intervention. Here, we report a successful Aortic Root Replacement (ARR) and Total Arch Replacement (TAR) in an Arg179His ACTA2 mutation patient with severe cerebral artery stenosis requiring intraoperative efforts.
Case report
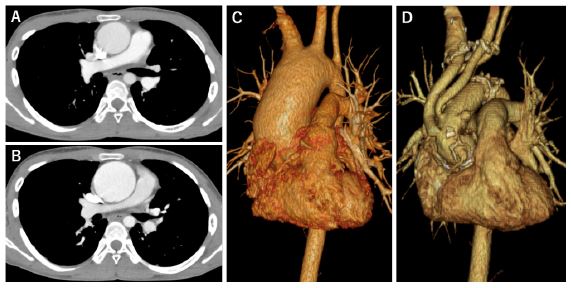
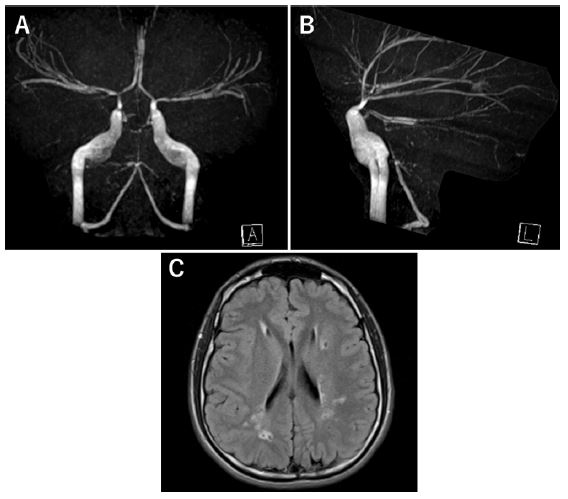
A 19-year-old male, diagnosed with an Arg179His ACTA2 mutation at an early age, had patent ductus arteriosus, bilateral intracranial artery stenosis, bilateral dilated pupils and loss of light reflex. He previously presented with Transient Ischemic Attacks (TIA) due to severe intracranial artery stenosis. Routine Computed Tomography (CT) surveillance against aortic aneurysmal formation discovered an abrupt dilatation of the aortic arch and ascending aorta at age 19. The ascending aorta enlarged from 40 mm (Figure 1A) to 53 mm (Figure 1B) in diameter over 15 months (Figure 1C). Since annuloaortic ectasia and moderate aortic regurgitation were also revealed, ARR, in addition to TAR, was planned. However, severe stenosis of the bilateral cerebral arteries and multiple, chronic cerebral infarctions (Figure 2) mandated strict operational planning, focused on prevention of complications.
TAR was performed first with cardiopulmonary bypass initiation via right axillary arterial graft cannulation and right atrial venous cannulation before moderate hypothermic circulatory arrest at 22°C and selective Antegrade Cerebral Perfusion (ACP). Right ACP was done from right axillary artery grafting and left ACP was done from a selectively cannulated left common carotid artery and left subclavian artery. Uninterrupted cerebral circulation was achieved by seamless perfusion from right axillary artery graft cannulation. Cerebral artery stenosis necessitated an ACP flow boost to 15 ml/kg/min to assure sufficient cerebral supply. TAR was performed using 24 mm Triplex quadrifurcated grafts (Terumo Corp., Tokyo, Japan). Subsequently, ARR was performed via Bentall procedure using a composite graft of a 21 mm Regent mechanical valve (Abbott, Illinois, USA) plus a 24 mm Gelweave Valsalva graft (Terumo Aortic, Renfrewshire, UK). Cerebral oximetry did not drop during the entire procedure. No post-operative neurological or cardiovascular complications were noted.
Discussion & conclusion
The Arg179His ACTA2 mutation is the most severe of its category because of very early onset and highly penetrant vascular diseases in affected patients [1]. However, since the first descriptions in 2010, operative outcomes of arch reconstruction for Arg179His mutations remain poorly reported. While Yetman et al. reported operative outcomes of three Arg179His mutation cases and described the malignancy of this disease [2], studies detailing aortic root and arch reconstruction and operative risks for this condition are persistently underreported.
Since aortic aneurysms associated with ACTA2 mutations involve the aortic root and ascending aorta, often extending into the arch over time, concomitant aortic arch replacement is a distinct eventuality [3]. In our case, although the aortic root and ascending aorta were the center of the dilation, the aortic arch was also replaced based on the described treatment policy. As such, staging with an elephant trunk is recommended as preparation for descending aorta replacement, as it often gradually enlarges [4]. However, in our case, the insufficient diameter of the descending aorta proscribed an elephant trunk and, instead, arch graft branches were placed proximally so that distal arch grafts can be easily manipulated for possible future descending aortic replacement.
Cerebral involvement is a hallmark of this disease, as 77% of patients with Arg179His ACTA2 mutations have intracranial artery stenosis or occlusion and 95% present hyperintensities in periventricular white matter on Magnetic Resonance Imaging (MRI) [4]. Cerebrovascular disease increases operational risks and therefore cerebral perfusion demands extreme vigilance during arch reconstruction. In this case, the patient had suffered from TIA since childhood and preoperative brain single photon emission computed tomography showed relative hypoperfusion in the left temporal lobe, indicating high stroke risk during TAR. Treatment for the hypoperfusion was considered prior to TAR. Direct and indirect cerebral revascularization are the main treatment options for ACTA2 cerebral arteriopathy, but success rates vary [5]. Therefore, we utilized uninterrupted continuous flow from axillary graft perfusion for initiation of selective ACP to minimize cerebral ischemic time. In addition, total ACP flow was increased to 15 ml/kg/min, while monitoring regional cerebral oxygen saturation, to prevent stroke.
Conclusion
We performed aortic root and arch replacement for aortic aneurysm in an Arg179His ACTA2 mutation patient. Increasing and continuous ACP flow is useful for preventing cerebrovascular complications from ACTA2 cerebral arteriopathy.
Declarations
Ethical statement: This study was approved by the institutional review boards of University of Tsukuba (IRB approval No. R04-065, 06/23/2022). The consent for publication was obtained from the patient and family.
Funding: The authors received no financial support for this article.
Conflict of interest: none declared.
Data availability statement: The data underlying this article will be shared on reasonable request by the corresponding author.
References
- Dianna M Milewicz, John R Østergaard, Leena M Ala-Kokko, et al. De Novo ACTA2 Mutation Causes a Novel Syndrome of Multisystemic Smooth Muscle Dysfunction. Am J Med Genet A. 2010; 152A(10): 2437-2443.
- Anji T Yetman, Lois J Starr, Steven B Bleyl, Lindsay Meyers, Jeffrey W Delaney. Progressive Aortic Dilation Associated With ACTA2 Mutations Presenting in Infancy. Pediatrics. 2015; 136(1): e262-6.
- Ellen S Regalado, Dong-chuan Guo, Siddharth Prakash, et al. Aortic Disease Presentation and Outcome Associated with ACTA2 mutations. Circ Cardiovasc Genet. 2015; 8(3): 457-64.
- Ellen S Regalado, Lauren Mellor-Crummey, Julie De Backer, et al. Clinical History and Management Recommendations of the Smooth Muscle Dysfunction Syndrome Due to ACTA2 Arginine 179 Alterations. Genet Med. 2018; 20(10): 1206-1215.
- Joshua A Cuoco, Christopher M Busch, Brendan J Klein, et al. ACTA2 Cerebral Arteriopathy: Not Just a Puff of Smoke. Cerebrovasc Dis. 2018; 46(3-4): 161-171.