Introduction
Metastatic spread to the spleen is rare for solid organ tumours and often is associated with widespread metastatic disease. Common primary sources included breast, colorectal, ovarian and melanoma. While the prevalence ranges between 2.3 and 7.1% in those with cancer examined at autopsy the percentage of those living with clinically significant splenic metastatic disease is much lower [1].
Oligometastatic disease to the spleen is even rarer with less than 100 cases reported up until 2007 [2]. The infrequency of splenic metastases is likely due to several anatomical and physiologic characteristics that makes it naturally resistant to neoplastic seeding. This includes the splenic capsule acting as a physical barrier, a tortuous splenic artery with continuous flow through the spleen and a lack of afferent lymphatics. The spleen’s role in immune regulation results in a high density of immune cells which produces a high concentration of angiogenesis inhibitor factor creating an antineoplastic environment [3,4].
There has been a growing trend towards resection of isolated metastatic deposits in certain cohorts such as colorectal cancer with isolated liver metastases and this has survival benefits. However, given the lack of cases that present with oligometastatic disease to the spleen there are no clear guidelines how it should be treated. The decision is therefore left down to individual clinicians to assess them on a case-by-case basis.
Herein we present the case of a 76-year-old man who was diagnosed with oligometastatic lung cancer with an isolated splenic metastasis that was treated with a laparoscopic splenectomy.
Case report
A 76-year-old man was referred to the surgical outpatient department by the medical oncologist for consideration of splenectomy.
He had been diagnosed with Non-Small-Cell Lung Cancer (NSCLC) 9 months prior and was treated with definitive chemoradiotherapy. Otherwise, his past medical history included hyperlipidaemia and diverticular disease. He was a fit individual with an ECOG status of 1. His initial post treatment staging scan showed a good response of his lung primary to the treatment but there was a new 15 mm splenic lesion. The lesion was indeterminant but there was concern it may reflect a metastasis hence he proceeded for an early surveillance PET CT scan to further define. In the 2 months between the CT and PET scan the lesion had further increased in size from 15 mm to 23 mm and exhibited moderate avidity consistent with a metastasis.
He was presented at the surgical oncology MDT meeting. Given the rarity of splenic metastasis there was concern occult metastatic disease might be present and the consensus was to proceed again with close surveillance imaging to assess stability of the lesion and ensure no further metastatic disease was developing that would preclude him from surgical intervention.
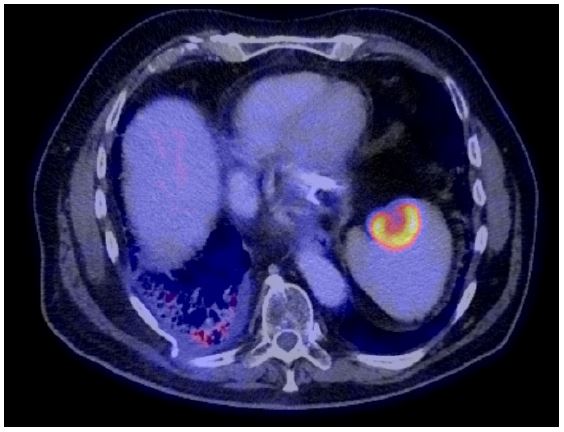
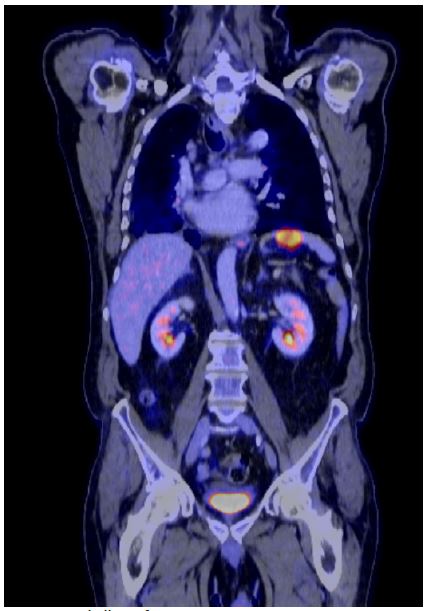
A second PET CT was done 2 months later which demonstrated the lesion had further increased to 33 mm (FIgures 1 & 2). Again, there was no evidence of other metastatic disease. Given the increasing size with disruption of the splenic capsule decision was for discussion of splenectomy not only as treatment of the presumed oligometastatic disease but prevention of splenic rupture.
The patient was entirely asymptomatic of the lesion but was keen to proceed given he had a good quality of life and functional status. He received his preoperative vaccinations and was booked for an elective laparoscopic splenectomy.
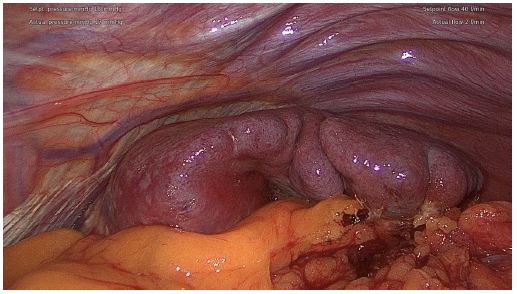
The operation proceeded and was completed laparoscopically (Figures 3 & 4). A drain was left as the pancreatic tail was adhered onto the spleen, but it was dissected free without injury. He was admitted to the ward and observed for 2 days as an inpatient. He was discharged with the drain in-situ and reviewed in the outpatient clinic 7 days later to have it removed. His final histology demonstrated a 40 mm deposit of non-small cell lung cancer. He has now recovered well from the operation and continues with active surveillance of his lung cancer.
Discussion
Metastatic NSCLC has a median survival of 12 months with chemotherapy but with immunotherapy such as pembrolizumab survival is increased up to 20 months [5]. Splenic metastases from NSCLC occur in 0.66% of cases [6]. The role of surgery in metastatic disease is limited however one trial explored surgery or ablative radiotherapy for metastases in combination with additional immunotherapy and found it offered a progression-free survival benefit of 12.5 months [7].
Radiotherapy could be considered as opposed to surgery. A systematic review of 486 patients treated with radiotherapy for splenomegaly secondary to haematological malignancies found it offered a significant reduction in patient pain and overall size of the spleen [8]. However, radiotherapy does not come without risk and one case report describing splenic rupture follow radiotherapy and the authors raised the suggestion of upfront splenectomy in suitable candidates over radiotherapy due to eventual risk of rupture [9].
The benefits of splenectomy should be balanced against the risk of post operative infections. Overwhelming Post-Splenectomy Infections (OPSI) reflect a rare but significant complication following splenectomy. The most common causative pathogens include S. pneumoniae, N. meningitidis and H. influenzae and while prophylactic antibiotics and vaccinations play a key role the risk of sepsis is lifelong [10]. This risk is further increased in patients with metastatic disease who require further adjuvant therapies which further impairs their immune system.
There have been several publications describing splenectomy for the treatment of splenic metastases of various cancers. All have suggested this conferred a survival advantage to the patient by treating the disease and should be considered in other patients [11,12].
Conclusion
Isolated metastatic disease of the spleen is rare. This case highlights that splenectomy can be considered not only for treatment of the disease but prevention of progression and eventual rupture which becomes a surgical emergency. Given the rarity of its presentation any occult metastatic disease should be excluded first which may dictate alternative treatment pathways.
Conflict of interest: The authors declare no conflicts of interest
Funding: There was no funding received for this case report. It was entirely self-funded by the authors.
References
- Berge T. Splenic metastases: Frequencies and patterns. Acta Pathol Microbiol Scand. 1974; 82: 499-506.
- Comperat E, Bardier-Dupas M, Camparo P, Capron F, Charlotte F. Splenic metastases: Clinicopathologic presentation, differential diagnosis, and pathogenesis. Arch Pathol Lab Med. 2007; 131: 965-969.
- Tang H, Huang H, Xiu Q, Shi Z. Isolated splenic metastasis from lung cancer: ringleader of continuous fever. European Respiratory Review. 2010; 19(117): 253-256.
- Warren S, Davis AH. Studies on tumour metastasis: The metastases of carcinoma to the spleen. Am J Cancer. 1934; 21: 517-533.
- Mok TSK, Wu YL, Kudaba I, Kowalski DM, Cho BC, et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressign locally advances or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, phase 3 trial. Lancet. 2019; 393(10183): 1819-1830.
- Niu FY, Zhou Q, Yang JJ, Zhong WZ, Chen ZH, et al. Distribution and prognosis of uncommon metastases from non-small-cell lung cancer. BMC Cancer. 2016; 14: 149.
- Bauml JM, Mick R, Ciunci C, Aggarwal C, Davis C, et al. Pembrolizumab after completion of locally ablative therapy for oligometastatic non-small-cell lung cancer: a phase 2 trial. JAMA Oncol. 2015; 5: 1283-1290.
- Naorsky NG, Williams GR, Barta SK, Esnaola NF, Kropf PL, et al. Splenic irradiation for splenomegaly: A systematic review. Cancer Treat Rev. 2017; 53: 47-52.
- Chen RJ, Gillespie C, Rowcroft A, Knowles B. Splenectomy for ruptured non-small cell lung cancer metastasis: an unusual indication. ANZ J Surg. 2021; 91(5): 332-334.
- Di Sabatino A, Carsetti R, Corazza GR. Post-splenectomy and hyposplenic states. Lancet. 2011; 378: 86-97.
- Lopez MJ, Targarona SE, Peraza SY, Yidal GP, Balague PC, et al. Laparoscopic approach for isolated splenic metastasis: Comprehensive literature review and report of 6 cases. Surg Laparosc ENdosc Percutan Tech. 2013; 23(1): 21-24.
- Lopera CA, Vergnaud JP, Matutue-Turizo G, Pereira-Warr S, Laparoscopic splenectomy for splenic metastasis from primary lung carcinoma. Case Rep Surg. 2018: 2620301.