Introduction
First described in 1924 by Libman Sacks [1], and characterized by verrucous lesions of the heart valves and the presence of small aseptic vegetations, Libman Sacks Endocarditis (LSE) is a characteristic cardiac manifestation of Systemic Lupus Erythematosus (SLE) [2]. 61% of patients with SLE have valvular involvement [3].
In their series of 69 lupus patients, Roldan et al. found a 43% prevalence of Libman-Sacks endocarditis with systematic Trans Esophageal Echocardiography (TEE) [4]. In contrast, other authors have found a prevalence of no more than 20% in lupus patients [5], a difference that may be explained by the fact that TEE is not routinely performed.
We report the case of a 52-year-old patient with SLE complicated by lupus nephritis who underwent mitral valve surgery.
Clinical case
A 52-year-old patient with SLE, complicated by lupus nephritis on prednisone, was diagnosed with dyspnea stages II and III of NYHA.
The clinical examination was done on a conscious patient, well oriented in time and space, with a general condition corresponding to stage 2 of the WHO Performance Status hemodynamically stable: blood pressure (BP)=110/60 mmHg/ heart rate (HR)=85 bpm/ saturation (SpO2)=97% on room air.
On auscultation, the cardiovascular examination revealed regular heart sounds as well as a systolic murmur in the mitral foci. Peripheral pulses, which are ample and bouncy, are perceived symmetrically.
Electrocardiogram demonstrated sinus tachycardia without other associated anomalies. Chest x-ray at admission showed mild cardiomegaly and bilateral basilar interstitial lung pattern.
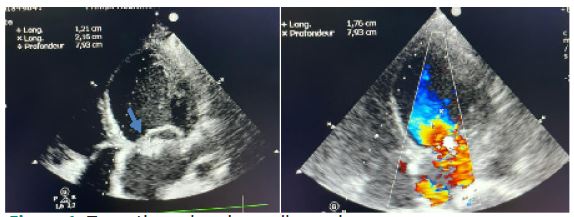
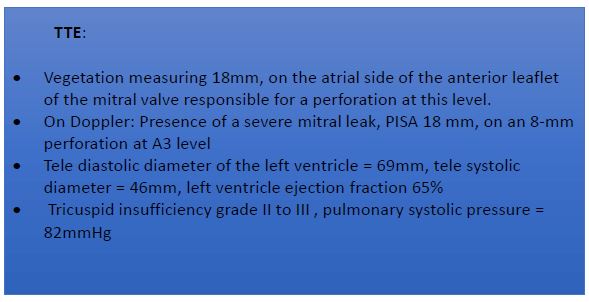
In view of this clinical picture, Transthoracic Echocardiography (TTE) was performed, which confirmed the significant mitral insufficiency and large mitral vegetation (Figure 1).
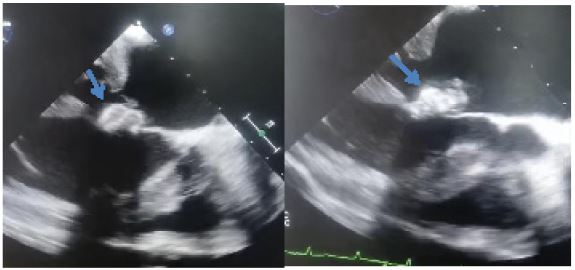
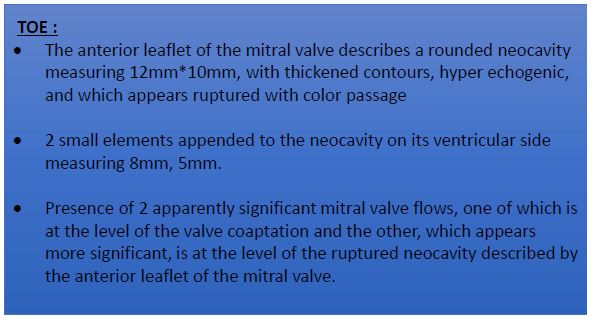
A TOE was used to complete the assessment in front of the MI and mitral vegetation (Figure 2).
Biological blood tests showed C reactive protein at 85, white blood cells 15000, and cytobacteriological examination of urine returned positive for Esherishia Coli. Blood cultures were negatives.
On the basis of this diagnosis, the patient was admitted to the operating theatre for surgical management.
Under general anesthesia, a vertical median sternotomy was performed, followed by the installation of a extracorporeal circulation, between aortic cannulation and cannulation of both vena cava, cardiac arrest occurred after administration of crystalloid cardioplegia via the anterograde route.
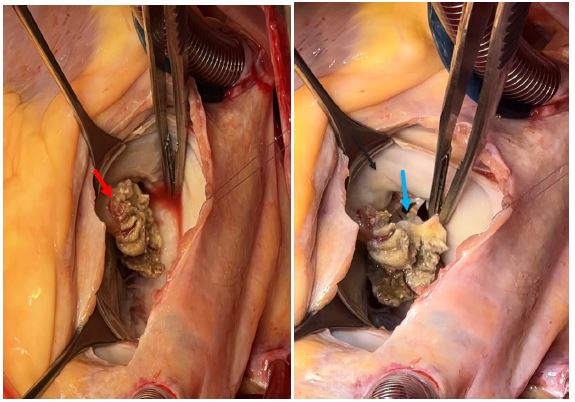
Exposure of the mitral valve through the opening of the right atrium, and the septum through the foramen ovale, revealing large vegetation raising suspicion of a degeriated abscess suspended on the atrial side of the anterior leaflet of the mitral valve between A2, A3, with a large perforation at this level
A careful and enlarged vegectomy was performed, and a mitral plasty was carried out, which was unsuccessful due to the fragility of the valve leaflets. Hence the decision to replace the mitral valve with a CARBOMEDICS n31 mechanical prosthesis after resection of the anterior leaflet, and the conservation of the posterior leaflet and the subvalvular apparatus.
Tricuspid annulopasty was performed with an EDWARDS n°32 ring.
Exit from bypass under positive inotropic drugs, after 87 min of bypass time and 62 min of clamping time.
The patient was extubated at H10, and the postoperative course was straightforward.
Patient anticoagulated with heparin and vitamin K antagonist.
Results and follow-up
• Bacteriological examination of the vegetation was nega- tive, while histological examination revealed a totally destroyed valve wall, replaced by eosinophilic fibrinous material showing multiple foci of calcification on an in- flammatory background in favor of infectious endocardi- tis in the course of organization.
• Haematological blood test for Lupus Anticoagulant (LA) was positive.
• A follow-up TTE after 1 month showed a mechanical pros- thesis in a well-functioning mitral position, with a mean gradient of 5 mmHg and no leakage, with an ejection frac- tion of 50%.
Discussion
Libman Sacks endocarditis, a form of Non-Bacterial Throm- botic Endocarditis (NBTE), is a well-known cardiovascular manifestation of SLE, with valvular thickening, vegetation formation and regurgitation being the main pathological features [3].
When medical management fails to control symptoms or prevent complications, surgical intervention becomes necessary.
The decision between Mitral Valve Replacement (MVR) and mitral valve repair is influenced by multiple clinical, anatomical and patient-related factors.
Lesions mainly affect the mitral and aortic valves, but all four valves and the entire endocardial surface can be affected [6].
TTE is the examination of choice for diagnosing SLE, with the incidence of valvular heart disease varying between 18-50% [5,7,8] and increases to 74% if TEE is performed [9].
Valvular lesions are characterized microscopically by fibrin deposits, an infiltrate of mononuclear inflammatory cells, fibrosis, neovessels and sometimes immunoglobulin and complement deposits [10,11].
The presence of Antiphospholipid Antibody Syndrome (APAS), found in our case by a positive LA blood test, is associated with a high prevalence of mitral vegetation, suggesting, according to studies by Khamashta MA et al, Gabrielli F et al, a pathogenic involvement of antiphospholipid antibodies.
Mitral valve surgery in SLE
• No consensus has yet been reached on this question, and data are limited to a small number of case reports and series of a few cases, so indications are not well studied. Surgical treatment is certainly indicated in cases of large vegetation, severe Mitral Insufficiency (MI) and recurrent thromboembolic events, even under medical treatment.
• Some authors, Hakim JP and al., Chauvaud SM and al, suggest that mitral valve replacement leads to better results than plasty [14,15], arguing that by the evolution of valve calcification and fibrosis in lupus and APAS leads to rapid recurrence of MI after plasty, necessitating further surgery. In addition, it has been reported that corticosteroid therapy indicated in the treatment of SLE can lead to narrowing of the heart valves [16], while the presence of APAS i
• In specific cases, Bouma et al [18] conclude that conservative surgical treatment is justified, particularly in young patients, if LES and/or APAS are stabilized on immunosuppressive therapy, and if intraoperative macroscopic examination shows suitable valve leaflet anatomy, with localized lesions, and mitral plasty appears feasible. And above all, in young women wishing to become pregnant, to avoid the need for anticoagulant treatment.
In our case, despite being a young patient with localized lesions in the anterior mitral valve, and thin flexible leaflets, a mitral valve repair was envisaged for reconstruction of the valve perforation and consolidation of the plasty. However, the fragility of the infiltrated and scarred tissue meant that the mitral valve had to be replaced by a mechanical prosthesis.
Conclusion
Early, multidisciplinary management of SLE can prevent its complications, which can be serious. In the event of surgical indication, the choice between mitral valve repair or replacement must meet clinical, anatomical and patient-related criteria.
References
- Libman E, Sacks B. A hitherto undescribed form of valvular and mural endocarditis. Arch Intern Med. 1924; 33: 701-37.
- Gross L. The cardiac lesions in Libman-Sacks disease with a consideration of its relationship to acute diffuse lupus erythematosus.
- Y Berkun, A Elami, K Meir, et al. Increased morbidity and mortality in patients with antiphospholipid syndrome undergoing valve replacement surgery, J. Thorac. Cardiovasc. Surg. 2004; 127: 414-420. http://dx.doi.org/10. 1016/j.jtcvs.2003.07.016.
- Roldan CA, Shively BK, Crawford MH. An echocardiographic study of valvular heart disease associated with systemic lupus erythematosus. N Engl J Med. 1996; 335(19): 1424- 30. PubMed | Google Scholar
- Galve E, Candell-Riera J, Pigrau C, Permanyer-Miralda G, Gar- cía del Castillo H, et al. Prevalence, morphologic types, and evolution of cardiac valvular disease in systemic lupus eryt- hematosus. N Engl J Med. 1988; 319: 817-23.
- Galve E, Ordi J, Candell J, Soler Soler J. Patología del corazón de origen extracardíaco (VI). Enfermedades del tejido conectivo y corazón. Rev Esp Cardiol. 1998; 51: 232-42.
- Cervera R, Font J, Paré C, Azqueta M, Pérez-Villa F, et al. Cardiac disease in sistemic lupus erithematosus: prospec- tive study of 70 patients. Ann Rheum Dis. 1992; 51: 156-9.
- Crozier IG, Li E, Milne M, Nichols G. Cardiac involvement in systemic lupus erithematosus detected by echocardiografhy. Am J Cardiol. 1990; 65: 1145-8.
- Roldan CA, Shivaly BK, Lau CC, Gurule FT, Smith EA, et al. Systemic lupus erithematosus valve disease by transe- sophageal echocardiografhy and the role of antiphospholipid anti- bodies. J Am Coll Cardiol. 1992; 20: 1127-34.
- Piette JC, Lê Thi Huong Du, Laraki R, Cacoub P, Chapelon C, et al. Les valvulopathies des connectivites [Valvulopathies in connectivitis]. Ann Med Interne (Paris). 1992; 143(4): 251-6. French. PMID: 1444007.
- Doherty NE, Siegel RJ. Cardiovascular manifestations of systemic lupus erythematosus. Am Heart J. 1985; 110(6): 1257-65. doi: 10.1016/0002-8703(85)90023-7. PMID: 3907317.
- Khamashta MA, Cervera R, Asherson RA, Font J, Gil A, et al. Association of antibodies against phospholipids with heart valve disease in systemic lupus erythematosus. Lancet. 1990; 335(8705): 1541-4. doi: 10.1016/0140-6736(90)91373-i. PMID: 1972484.
- Gabrielli F, Alcini E, Di Prima MA, Mazzacurati G, Masala C. Cardiac valve involvement in systemic lupus erythematosus and primary antiphospholipid syndrome: lack of correlation with antiphospholipid antibodies. Int J Cardiol. 1995; 51(2): 117-26. doi: 10.1016/0167-5273(95)02357-3. PMID: 8522406.
- Hakim JP, Mehta A, Jain AC, Murray GF: Mitral valve replacement and repair. Report of 5 patients with systemic lupus erythematosus. Tex Heart Inst J. 2001; 28: 47-52.
- Chauvaud SM, Kalangos A, Berrebi AJ, Gaer AR, Acar C, et al. Systemic lupus erythematosus valvulitis: mitral valve replacement with a homograft. Ann Thorac Surg. 1995; 60: 1803-5.
- Hoffman R, Lethen H, Zunker U, et al. Rapid appearance of severe mitral regurgitation under high-dosage corticosteroid therapy in a patient with systemic lupus erythematosus. Eur Heart J. 1994; 15: 138-9.
- Gordon RJ, Weilbaecher D, Davy SM, et al. Valvulitis involving a bioprosthetic valve in a patient with systemic lupus erythematosus. J Am Soc Echocardiogr. 1996; 9: 104-7.
- Bouma W, Klinkenberg TJ, van der Horst IC, et al. Mitral valve surgery for mitral regurgitation caused by Libman-Sacks endocarditis: A report of four cases and a systematic review of the literature. J Cardiothorac Surg. 2010; 5: 13.