Late seroma formation after implant removal
Theresa K Webster; Jeffrey A Ascherman*
New York Presbyterian Hospital Weill Cornell and Columbia University Irving Divisions of Plastic Surgery, NY, USA.
New York Presbyterian Hospital Weill Cornell and Columbia University Irving Divisions of Plastic Surgery, NY, USA.
Introduction: While Breast Implant-Associated Anaplastic Lymphoma (BIA-ALCL) was first recognized by the WHO in 2016 there has been limited information on this implant associated cancer due its limited incidence worldwide. Despite the lack of literature beyond case series and reports, the association between textured implants and this cancer has been well documented as has its typical presentation of a late seroma. Herein, we present a case report of a patient presenting similarly with a late seroma; however, the seroma occurred more than 20 years following implant removal.
Case Report: A 58-year-old female with PMH Raynaud disease presented with a chief complaint of persistent bilateral breast fullness along with a new inferior left breast collection following removal of her implants over 20 years prior. She initially had sub-pectoral smooth saline implants placed in June 2000 for augmentation but then developed capsular contracture for which she underwent capsule revision in June 2001 and then ultimately implant removal a few months later. Despite implant removal she had persistent fullness and new late seroma formation for which she underwent partial capsulectomies. Pathology was negative for CD30.
Conclusion: While late seroma has been identified as the hallmark clinical presentation of BIA-ALCL, this case report demonstrates late seroma formation in a patient who previously had smooth implants removed over 20 years prior and in whom her CD30 was negative. More information is needed to determine additional etiology of late seroma formation in the absence of malignancy.
Manuscript Information: Received: Jun 12, 2024; Accepted: Jul 24, 2024; Published: Jul 31, 2024
Journal: Annals of Surgical Case Reports & Images
Online edition: https://annscri.org
Copyright: © Ascherman JA (2024). This Article is distributed under the terms of Creative Commons Attribution 4.0 International License.
Cite this article: Webster TK, Ascherman JA. Late seroma formation after implant removal. Ann Surg Case Rep Images. 2024; 1(4): 1039.
While breast implant-associated anaplastic lymphoma (BIA-ALCL) was first recognized by the WHO in 2016 there has been limited information on this implant-associated cancer due its limited but wide range of reported incidence worldwide. The range of incidence documented in the literature has ranged from 1 in 355 to 1 in 30,000 patients with a single institution study at Memorial Sloan Kettering demonstrating an incidence of 1 in 559 in patients with textured implants (Nelson).
Despite the lack of literature beyond mainly case series and reports, the association between textured implants and this cancer has been well documented as has its typical presentation of a late seroma. Late seroma has been the most common physical exam finding as demonstrated in greater than 80% of patients (Di Pompeo). Textured implants are thought to play a role due to their generation of chronic inflammation and thus antigenic stimulation in this peripheral T-cell mediated lymphoma (Niraula). Pathological analysis of the seroma typically demonstrates CD30 positivity and ALK negativity in BIA-ALCL. More recently, another implant-associated malignancy has been garnering attention, BIA-SCC or breast-implant associated squamous cell carcinoma. It presents similarly to BIA-ALCL with late seroma formation, but has positive markers for p63, CK5, and CK6 and has been demonstrated in patients with both smooth and textured implants (Niraula). Flow cytometry demonstrates atypical T cells in the case of BIA-ALCL and squamous cells in BIA-SCC. Treatment, as guided by the ASPS, of both of these malignancies involves en bloc capsulectomy.
With both of these malignancies, patients typically present with late seroma formation in the setting of retained implants. However, herein we present a case report of a patient presenting with a late seroma more than 20 years following implant removal.
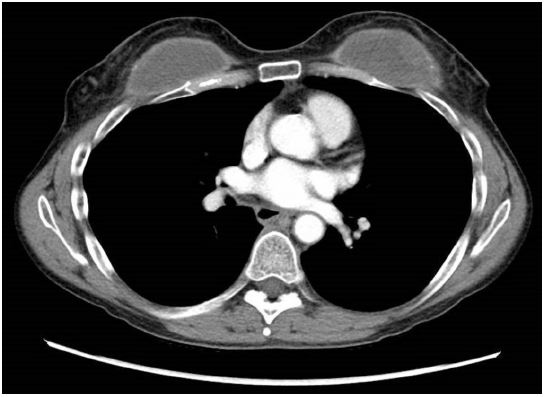
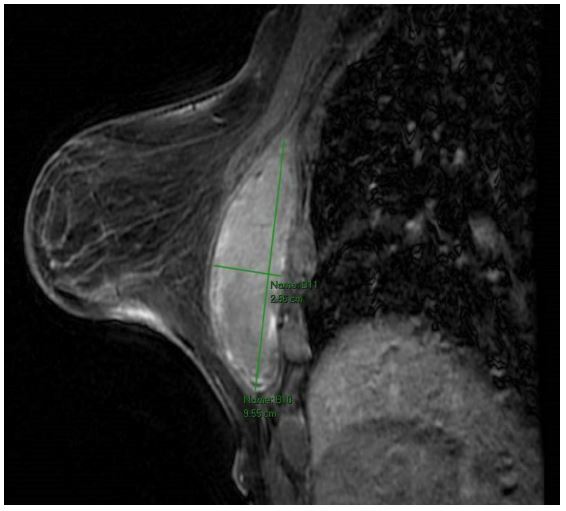
A 58-year-old female with PMH Raynaud disease presented with a chief complaint of persistent bilateral breast fullness along with a new inferior left breast collection following removal of her implants over 20 years prior (Figure 1). She initially had sub-pectoral smooth saline implants placed in June 2000 for augmentation but then developed capsular contracture for which she underwent capsule revision in June 2001 and then ultimately implant removal a few months later. She did not undergo any further breast surgeries or procedures from the time of implant removal to presentation. She also denied any recent breast trauma. Given this new inferior breast collection, she presented first to a breast surgeon who attempted unsuccessfully to aspirate the collection. The breast surgeon then sent her for CT, and despite having had her implants removed in 2001, her imaging was read as having intact implants (Figure 2). Breast MRI though correctly demonstrated bilateral breast capsules filled with hemorrhagic/proteinaceous material along with the inferior left breast collection. She had no personal or family history of breast cancer and the most recent mammogram two months prior to presentation was BI-RADS 3 and demonstrated bilateral intracapsular seromas.
Given these findings of persistent capsules with new seroma formation she was taken to the operating room for partial capsulectomies (Figure 4). Capsulectomies were performed in partial fashion due to the adherence of the capsules to her chest wall and ribs. Both capsules contained a dark brown, proteinaceous fluid with almost sludge-like consistency while the inferior collection contained a thinner, similarly colored brown fluid (Figure 5). The capsules were sent to pathology while the fluid was sent for immunohistochemistry, flow cytometry, cell count, and cytology.

Post-operatively, she recovered without complication and her capsules were negative for CD30 and *** for ALK, CK5/6, and p63 (need final path results). Cytology was notable for a lack of atypical lymphocytes.


While unilateral late seroma on average 7 to 10 years after implant placement is the most typical presentation for BIA-ALCL, this case report highlights a patient in whom late seroma formation occurred despite implant removal more than 20 years prior (ASPS) [1-6]. Notably, her capsules were almost entirely intact bilaterally at the time of capsulectomy and consistent with Baker grade 3 capsular contracture at the time of presentation. While BIA-SCC will often present with capsular contracture, it is seen less frequently with BIA-ALCL (ASPS). Capsular contracture in itself remains a complicated outcome following augmentation mammaplasty with theories pointing to bacterial contamination, trauma, blood, and implant content contamination (Boyd). Of note, current guidelines for treatment of BIAALCL and BIA-SCC recommend en-block capsulectomy at the time of implant removal given the risk of cancer recurrence and lower survival in patients with retained capsules (Longo). Luckily for this patient her capsule pathology was negative for the typical markers for both BIA-ALCL and BIA-SCC and her cytology did not demonstrate any malignant cells; however, the question remains as to why she had late seroma formation more than 20 years after implant removal. She denied any recent breast surgeries, procedures, or trauma, and unlike BIA-ALCL or BIA-SCC she presented with bilateral intra-capsular seromas. Additional research is needed to determine additional etiologies of late seroma formation aside from malignancy.
Financial disclosures: None.