Case description
A preterm male newborn was being treated in the neonatal intensive care unit for sepsis (staphylococcus epidermidis),
bronchopulmonary dysplasia and an intraventricular hemorrhage. He was born by an emergency cesarean section after
placenta abruption, at 24 weeks and 4 days of gestation. Birth
weight was 780 g. He was on enteral and parenteral feeds. He
was kept under mechanical intermittent positive pressure ventilation since birth.
On the 12th day of life, the patient presented with respiratory
instability, demanding higher levels of FiO2
, and regular ventilatory parameters adjustments. The surgical team was called to
evaluate a mild abdominal distention. During physical examination, a distended but non tender abdomen was noticed, with
audible normal bowel sounds. Known bilateral inguinal hernias
were enlarged and difficult to reduce. Blood analysis showed no leukocytosis, normal platelet count and a normal C-reactive
protein level.
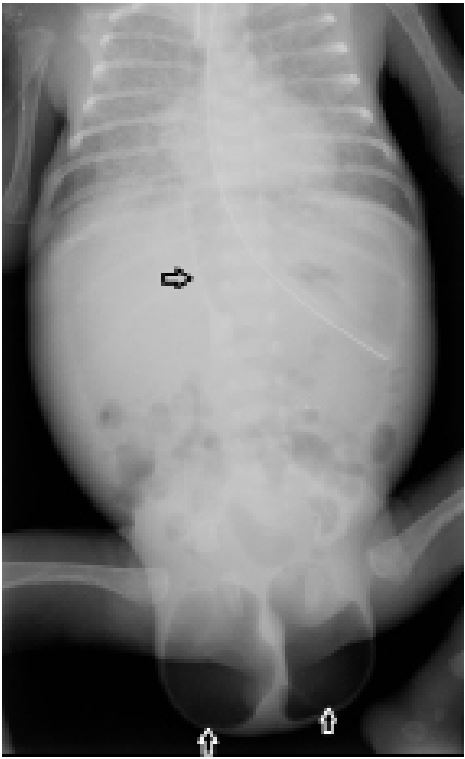
Plain radiographs showed two areas of radiolucency in the
scrotum indicating the presence of air, and a falciform ligament
sign.
Bowel perforation was suspected, and an exploratory laparotomy was performed: A single perforation was noted in the
terminal ileum, close to the ileocecal valve. The perforation
was closed with interrupted suture, and an ileostomy was performed proximal to the suture.
Two months later, the patient underwent ileostomy reversal
and bilateral correction of the inguinal hernias. The first year of
follow-up was uneventful [1-4].
Consent: A written informed consent has been obtained
from the guardian of the patient for the publication of this case.
References
- Angurana SK, Kanojia RP, Peruri G, Sundaram V. Pneumoscrotum
as a presentation of necrotising enterocolitis. BMJ Case Rep.
2018; 2018.
- Cochetti G, Barillaro F, Cottini E, D’Amico F, Pansadoro A, et al.
Pneumoscrotum: Report of two different cases and review of
the literature. Ther Clin Risk Manag. 2015; 11: 581-7.
- Dagur G, Lee MY, Warren K, Imhof R, Khan SA. Critical Manifestations of Pneumoscrotum. Curr Urol. 2016; 9(2): 62-6.
- Koh CC, Sheu JC. Intestinal atresia presenting as bilateral scrotal
pneumatocele: A case report. J Pediatr Surg. 2002; 37(1): E2.