Introduction
In adults, teratomas are rarely found extra-gonadally. Benign
mediastinal teratomas are ever rarer, with only 108 reported
cases from January 1992 to January 2018 [1]. Of all germ cell
tumors, mediastinal tumors only represent around 1-3% of
germ cell neoplasms [2]. Teratomas are histologically defined
as containing tissue from all three germ cell layers including
the endoderm, mesoderm, and ectoderm. Mature teratomas
generally present with well-differentiated germinal derivatives
in comparison to immature teratomas where differentiation of
germinal derivatives is less clear [3]. Herein, we report a case of
successful robotic surgical management of an anterior mediastinal mature teratoma in an adult.
Case presentation
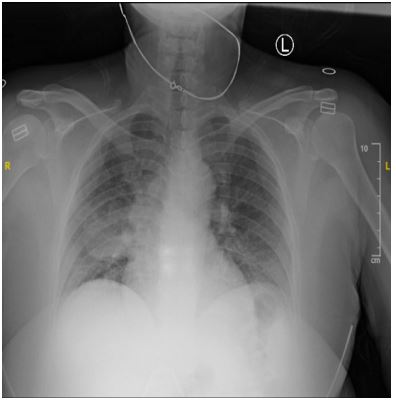
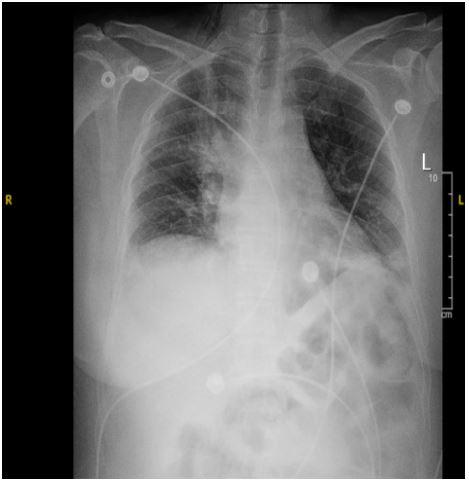
A 43-year-old female presented to the emergency department with a productive (non-bloody) cough and non-radiating
substernal right-sided chest pain for the prior six days. An initial
radiograph showed a 4.4 cm right midlung opacity (Figure 1).
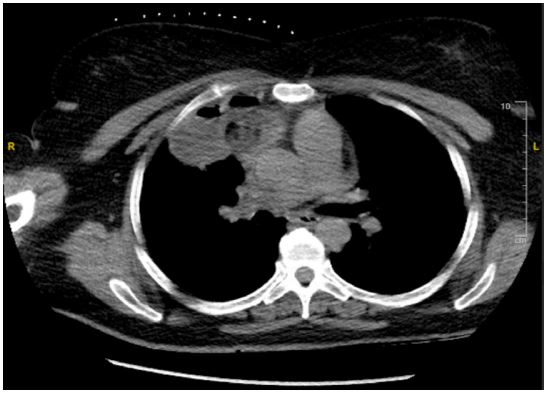
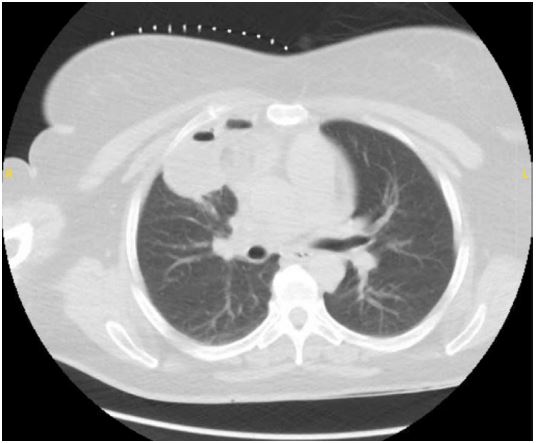
An initial computerized tomography scan showed a 7.8 cm invasive right upper lobe mass that invaded the mediastinum. Histopathology of a subsequent computerized tomography-guided
right lung biopsy showed organizing fibrosis and granulomatous
inflammation and scattered foreign body type multinucleated
giant cells and rare non-necrotizing epithelioid granuloma, but
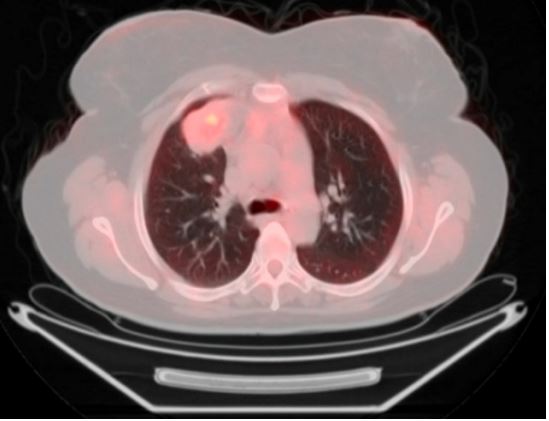
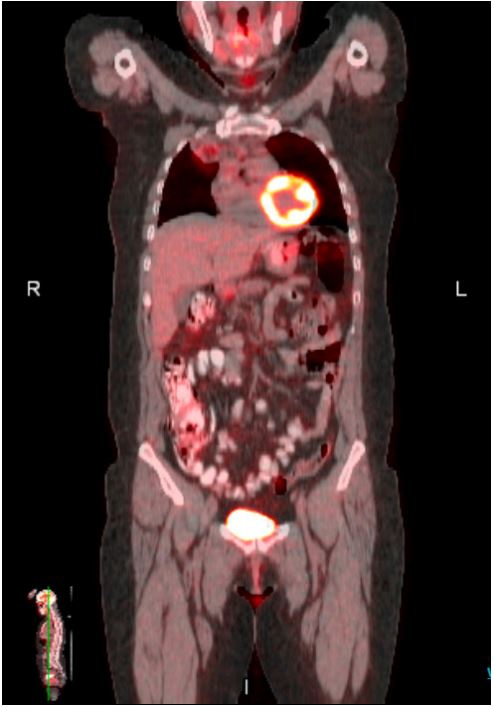
was inconclusive for a diagnosis of a specific entity. Positron
emission tomography scan showed a 3.7 cm x 6.5 cm x 3.4 cm
hypermetabolic (standardized uptake value max = 6.0) heterogenous right upper lobe mass extending into the right anterior
mediastinum. Her past medical history was significant for migraines. Physical exam was notable for bilateral lower leg edema. After presentation at our multidisciplinary conference, the
decision was made to proceed with robotic surgical resection.
Intra-operatively, the right upper lobe was found to have adhesions to the mediastinum. These adhesions were taken down
with bipolar cautery. The mediastinal mass was then shelled
out and a cavity was noted in the lung. The cavity was partially
excised with Bovie, sharp dissection, and blunt squeezing of
the cavity’s granulomas. Intraoperative frozen biopsy showed
skin and adnexal tissue compatible with teratoma. The cavity of the right upper lobe was then wedged out using a green
load ECHELON™ 3000 Stapler (ETHICON, Inc., Raritan, NJ). The
lungs were re-inflated under direct vision and two chest tubes
were inserted. After ensuring successful lung re-inflation and
hemostasis, all incisions were closed, and the patient was extubated and transferred to recovery without incident. The chest
tubes were taken out on post-operative day two. The rest of
the post-operative course was uneventful, and the patient was
discharged home on post-operative day four.
Discussion
Most benign mediastinal teratomas are discovered due
to symptoms such as chest pain, cough, and breathlessness,
although some can be asymptomatic and are incidental findings on chest radiography. Patients with mediastinal germ cell
tumors also rarely have abnormal physical findings. In some
cases, especially when the neoplasm is malignant, there may
be significant levels of human chorionic gonadotropin or alphafetoprotein [4]. When a symptomatic mediastinal teratoma is
suspected, the only curative and mainstay of treatment is surgical resection, which usually results in the complete resolution
of symptoms without the need for chemotherapy or radiation.
It is important to excise mediastinal neoplasms to prevent potential invasion into the superior vena cava, development of
pleural effusions, or rupture into the pericardial cavity with the
potential to cause cardiac tamponade [5]. After excision, benign
mediastinal teratomas rarely reoccur [1]. Although historically
mediastinal teratoma resection has been performed open (for
larger and more invasive tumors) it has been shown that minimally invasive approaches with video-assisted thoracoscopic
surgery have comparable outcomes but with decreased morbidity and hospital length of stay when compared with median
sternotomy [6,7]. Our case has shown that robotic-assisted thoracoscopic resection is a feasible method for resection of mediastinal teratomas, even with invasion of the neoplasm into the
lung.
Conclusion
While there is no established consensus on the approach to
resection of mediastinal teratomas, there are not many cases
of robotic-assisted thoracoscopic resection published in the literature, and our case has shown that robotic-assisted thoracoscopic resection is a feasible method to resection of mediastinal
teratomas, even with invasion into the lung [8-10].
Declarations
Conflicts of interest: There are no conflicts of interest to disclose.
Funding: None.
Acknowledgements: Thank you to Lake Erie College of Osteopathic medicine for providing the funding for the 3D printer
and resin. Thank you to the Bon Secour Mercy Health St Elizabeth Emergency Medicine residents for participating in this
study. Thank you to Barbara Hileman, BA, CCRC, for assisting in
running statistical analysis.
References
- Tian Z, Liu H, Li S, Chen Y, Ma D, et al. Surgical treatment of benign mediastinal teratoma: Summary of experience of 108 cases. Journal of Cardiothoracic Surgery. 2020; 15(1): 36.
- Nichols CR. Mediastinal germ cell tumors. Clinical features and biologic correlates. Chest. 1991; 99(2): 472-9.
- Meghana P, Pradhan A, Dash M, Mohapatra D. A Rare Case of Anterior Mediastinal Mature Teratoma. Research and Reviews in Pediatrics. 2022; 23(1).
- Nichols CR. Mediastinal Germ Cell Tumors: Clinical Features and Biologic Correlates. Chest. 1991; 99(2): 472-9.
- Kang DK, Kang MK, Heo W, Hwang YH. Cardiac tamponade due to ruptured cystic teratoma: Report of two cases. Oxf Med Case Reports. 2021; 2021(6): omab044.
- Azenha LF, Deckarm R, Minervini F, Dorn P, Lutz J, et al. Robotic vs. transsternal thymectomy: A single center experience over 10 years. Journal of clinical medicine. 2021; 10(21): 4991.
- Pennathur A, Qureshi I, Schuchert MJ, Dhupar R, Ferson PF, et al. Comparison of surgical techniques for early-stage thymoma: Feasibility of minimally invasive thymectomy and comparison with open resection. The Journal of Thoracic and Cardiovascular Surgery. 2011; 141(3): 694-701.
- Ramcharran H, Wallen J. Robotic-assisted thoracoscopic resection of anterior mediastinal cystic teratoma: A case report and literature review. Journal of Cardiothoracic Surgery. 2022; 17(1): 67.
- Zheng R, Devin CL, O’Malley T, Palazzo F, Evans NR. 3rd. Surgical management of growing teratoma syndrome: Robotic-assisted thoracoscopic resection of mediastinal teratoma. Surg Endosc. 2020; 34(2): 1019-23.
- Mortman KD, Chaffee SB. Robotic-assisted thoracoscopic resection of a benign anterior mediastinal teratoma. Journal of Robotic Surgery. 2013; 7(4): 401-3.