Background
Gallbladder volvulus, or torsion, is rare and occurs when the
gallbladder twists on its longitudinal axis by more than 180 degrees, causing occlusion of the cystic vessels and duct. The first
report of gallbladder volvulus was described in 1898 by Wendel
and was associated with cholelithiasis [1]. Although the exact
aetiology of gallbladder volvulus is unknown, it is likely to be
precipitated by anatomical variation of the gallbladder mesentery and changes to the surrounding tissues with advancing
age [2]. Contrary to Wendel’s case, there does not seem to be a
correlation with cholelithiasis as only 32% of patients with the
condition have gallstones at the time of presentation [2].
We present a case of gallbladder volvulus in a 73-year old
woman who was rapidly diagnosed with the aid of Computed
Tomography (CT) and underwent successful early surgical intervention.
Case presentation
A 73-year old woman presented to the Emergency Department with a seven-hour history of sudden onset, severe upper
abdominal pain, waking her from sleep and associated with
vomiting. There were no historical symptoms suggestive of gallstone disease and an ultrasound scan four years previously demonstrated a normal gallbladder. The patient had a past medical
history of polymyalgia rheumatica, on low dose prednisolone,
and was a living kidney donor having undergone left nephrectomy 14 years previously. The patient had also experienced a
one stone weight loss over the preceeding few months, which
was attributed to a recent bereavement; she had a body mass
index of 19.93 kg/m2
. On arrival to the Emergency Department,
the patient was systemically well and routine observations were
within normal parameters. On examination, there was mild tenderness in the epigastrium without signs of peritonitis.
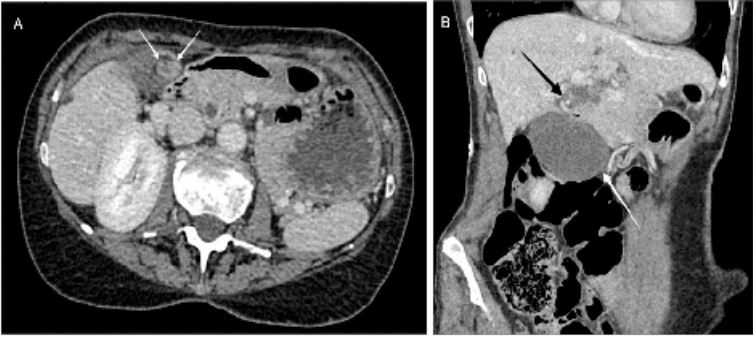
Blood tests demonstrated a slightly elevated C-Reactive Protein (CRP) of 20 mg/L, but were otherwise unremarkable, including liver function tests and amylase. A CT abdomen and pelvis with intravenous contrast was performed in the Emergency
Department, which revealed mural thickening and oedema of
the gallbladder along with poor enhancement. In addition, the
gallbladder had a relatively horizontal lie, with the fundus pointing medially and associated swirling of the vessels just outside
the hilum of the liver (Figure 1); a diagnosis of gallbladder volvulus was made
The patient was admitted under the care of the Hepatopancreatobiliary team and managed conservatively overnight. The
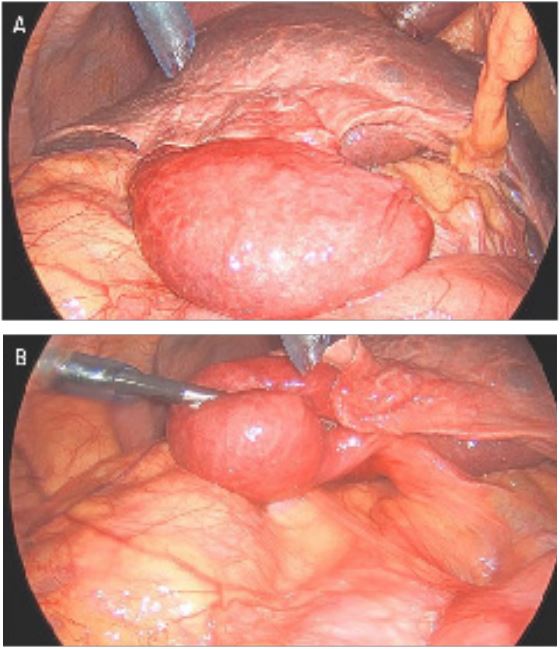
following morning, the patient underwent an urgent laparoscopic cholecystectomy. The operative findings were of a thickwalled gallbladder with a transverse lie (Figure 2a). The cystic
duct and artery were torted and within a long gallbladder mesentery (Figure 2b). The gallbladder was corrected into its usual
anatomical position before proceeding to a conventional laparoscopic cholecystectomy, beginning with fundal dissection.
The patient made an uncomplicated recovery and was discharged the following day. She remains well at 15 months post
procedure. Postoperative histology of the gallbladder reported
a congested gallbladder wall with haemorrhage. There was no
evidence of dysplasia or malignancy, and no reported cholelithiasis.
Discussion
The difficulty in diagnosing gallbladder volvulus preoperatively comes from the lack of specific symptoms, which may
mimic those of alternative gallbladder disease. However, with
a high level of suspicion, the clinician may elicit some important details to aid diagnosis. The condition usually occurs in elderly women, with a female: male ratio of 3:1 and median age
of 77 years [2]. As demonstrated in the above case, the patient
is likely to report sudden onset pain rather than an insidious
onset as with typical acute cholecystitis or intermittent pain as
with biliary colic. Early vomiting and remaining systemically well
at presentation are also common features [3]. Another patient
characteristic is a thin body habitus as loss of visceral fat may
precipitate gallbladder torsion in those with anatomical predispositions by elongating the gallbladder mesentery and reducing supporting surrounding tissues [3]. Interestingly, the patient
above demonstrates the common demographics and had recently experienced a sudden weight loss.
Mortality in this condition is quoted at around six percent
and is higher in those with delayed diagnosis and treatment [2].
Unlike acute cholecystitis, gallbladder volvulus is not amenable
to conservative management as twisting of the cystic artery
will lead to gallbladder ischaemia with eventual necrosis, perforation and biliary peritonitis. It is not uncommon for elderly
patients with acute cholecystitis to be managed conservatively,
owing to higher perioperative risks, however, in the case of gallbladder volvulus conservative management is likely to lead to a
poorer prognosis, so early surgical intervention should be mandated if the patient is fit to undergo the procedure.
Prompt CT scanning of patients in whom gallbladder volvulus
is suspected should be facilitated. Whilst some features seen
on CT may also be seen in acute cholecystitis, three features
have been proposed as a strong indicator for underlying volvulus when seen in combination: gallbladder distension; the presence of a twist along the gallbladder vascular pedicle; and an
abnormal lie of the gallbladder from vertical to horizontal [4].
Where possible, comparison to previous imaging is also of crucial importance to demonstrate a change in anatomy.
Conclusion
Gallbladder volvulus is an important differential diagnosis
to consider in patients presenting with upper abdominal pain.
Many of the differential diagnoses may be conservatively managed, thus the clinician must have a high level of suspicion for
gallbladder volvulus to facilitate early operative management
and therefore avoid the complications of gallbladder necrosis,
perforation and biliary peritonitis. The authors would advocate
a low threshold for imaging with CT, as an adjunct to diagnosis,
in order to limit delays in definitive treatment and reduce mortality.
References
- Wendel AV. VI. A Case of Floating Gall-Bladder and Kidney complicated by Cholelithiasis, with Perforation of the Gall-Bladder.
Ann Surg. 1898; 27(2): 199-202.
- Reilly DJ, Kalogeropoulos G, Thiruchelvam D. Torsion of the gallbladder: A systematic review. HPB (Oxford). 2012; 14(10): 669-
72.
- Lau WY, Fan ST, Wong SH. Acute torsion of the gall bladder in
the aged: A re-emphasis on clinical diagnosis. ANZ J Surg. 1982;
52(5): 492-4.
- Layton B, Rudralingam V, Lamb R. Gallbladder volvulus: It’s a
small whirl. BJR Case Rep. 2016; 2(3): 20150360.