Case report
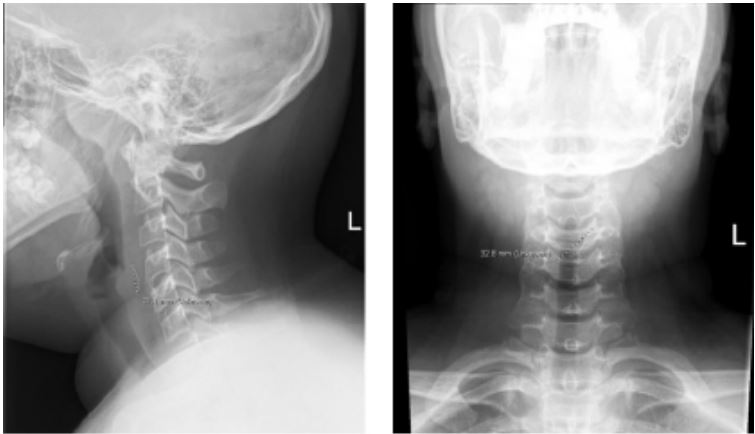
A 13-year-old male presented to the emergency department
following an episode of gagging while eating grilled chicken. He
reported significant odynophagia and globus sensation. He had
no symptoms of airway compromise. Neck radiograph was obtained which demonstrated a curvilinear radiopaque structure
measuring 3.2 cm in the region of the piriform sinus, presumed
to be a chicken bone given the history (Figures 1-2). ENT was
consulted and flexible laryngoscopy was performed. No foreign
body was identified.
The patient was taken to the OR for airway exam, esophagoscopy, and foreign body removal. Intraoperatively, there was
a small area of edema in the postcricoid region with a small
mucosal entry point. This was palpated with a right angle and a
small amount of purulence was expressed. The right angle was
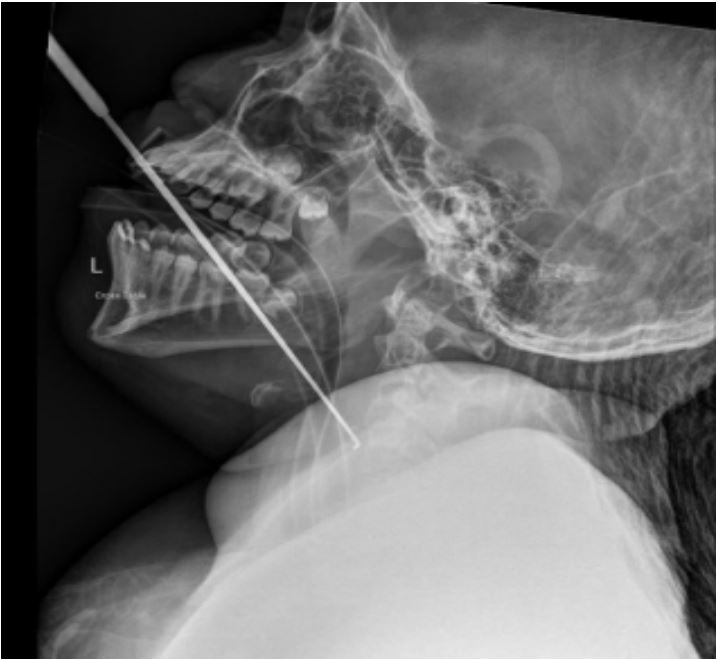
used to probe the wound, confirming the presence of a tract. To
localize the foreign body, an ETT was placed into the esophagus
and the right angle was positioned within the entry point while
an intraoperative x-ray was obtained (Figure 3). This confirmed
the location of the foreign body within the posterior esophageal mucosa. The microscope was brought into the room to allow for two-handed instrumentation. A sickle knife was used
to make a vertical incision in the posterior esophageal mucosa.
A combination of scissors, sickle knife, right angle, and suction
were used to dissect and probe the wound. Precise localization
of the object was difficult due to its small size. To aid in localization, a magnet was fashioned to the end of a nasogastric tube
and used to co-localize the magnetic foreign body within the
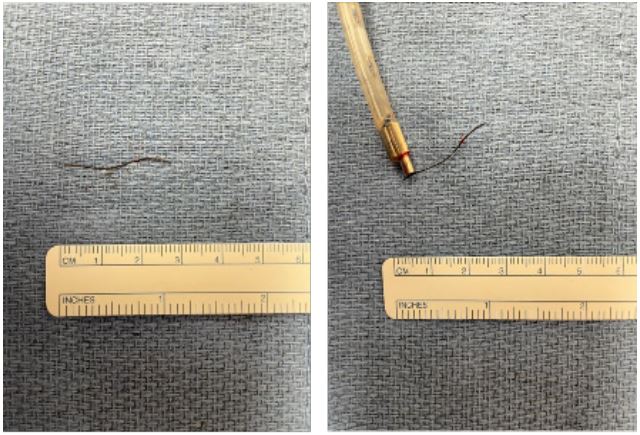
posterior esophageal mucosa. Once the foreign body was visible within the wound, alligator forceps were used to grab and
remove the foreign body. The foreign body was consistent with
a grill brush bristle measuring 2.8 cm (Figure 4-5).
A dobhoff tube was placed in the operating room, and the
patient was admitted overnight for observation. He underwent
a barium esophagram on post-operative day 1 with no evidence
of esophageal leak, and he was subsequently discharged home.
Discussion
Foreign bodies which are sharp may become embedded
within the upper aerodigestive tract when ingested. While this
is a relatively benign complication of foreign body ingestion,
it can lead to serious complications including retropharyngeal
abscess, esophageal perforation, or migration into the mediastinum with associated mediastinitis. One review notes bristle
migration occurring in 21% of upper aerodigestive tract cases
after initial presentation (Miller et al. 2021) [1]. For this reason, prompt identification and removal of a retroesophageal
foreign body is crucial. Even with the use of preoperative and
intraoperative imaging, precise localization of the object may
be challenging. Grill brush bristle ingestion is a public health issue and carries a high risk of becoming embedded within the
soft tissue of the aerodigestive tract. The national weighted
estimate of patients evaluated in the emergency department
after wire bristle ingestion in America between 2002-2014 was
1,700 (Baugh, Hadley, and Change, 2016) [2]. Though the object
in this case was originally presumed to be a chicken bone based
on history, the appearance on intraoperative imaging led us to
suspect a grill brush bristle which prompted us to use a magnet
to aid in its localization.
The use of a magnet to remove metal foreign bodies from
the gastrointestinal tract is not an entirely novel concept. One
article describes the possibility of using a magnetic tube to remove metal foreign bodies, which can potentially be utilized
in the awake patient if the object is in the proximal esophagus
and not embedded (Choe and Choe, 2019) [3]. Another case we
found describes a technique in which a snared magnet is used
to endoscopically remove a nonembedded paperclip within the
stomach (Coash and Yu, 2012) [4]. However, to our knowledge,
intraoperative use of a magnet to aid in the localization of an
embedded metal foreign body within the esophageal wall has
not been previously described in the literature.
Naunheim describes a similar presentation of a grill brush
bristle embedded in the hypopharynx. They used suspension,
microscope, and localized intraoperative fluoroscopy (2015) [5].
While intraoperative imaging is helpful for appropriate localization, we found that more accurate localization of the grill brush
bristle was accomplished with the addition of a magnet to this
technique. In hindsight, if we had employed the magnet earlier
in the case, we may have been able to identify the object prior
to obtaining intraoperative imaging and could have potentially
avoided unnecessary radiation.
Conclusion
Grill brush bristles may unknowingly be ingested and become embedded within the aerodigestive tract. Magnets are a
useful adjunct tool that can aid in both the intraoperative localization and removal of grill brush bristles and other metal
foreign bodies.
References
- Miller N, Noller M, Leon M, Moreh Y, Watson NL, et al. Hazards
and management of wire bristle ingestions: A systematic review.
Otolaryngology-Head and Neck Surgery. 2021; 167(4): 632-644.
- Baugh TP, Hadley JB, Chang CW. Epidemiology of wire‐bristle
grill brush injury in the United States, 2002‐2014. Otolaryngology-Head and Neck Surgery. 2016; 154(4): 645-649.
- Choe JY, Choe BH. Foreign body removal in children using Foley
catheter or magnet tube from gastrointestinal tract. Pediatric
Gastroenterology, Hepatology & Nutrition. 2019; 22(2):
132.
- Coash M, Wu GY. Endoscopic removal of a long sharp metallic
foreign body by a snared magnet: An attractive solution. Journal
of Digestive Diseases. 2012; 13(4): 239-241.
- Naunheim MR, Dedmon MM, Mori MC, Sedaghat AR, Dowdall
JR. Removal of a wire brush bristle from the hypopharynx using
suspension, Microscope, and fluoroscopy. Case Reports in Otolaryngology. 2015; 1-4.